Background: Transjugular intrahepatic portosystemic shunt (TIPS) creation is a commonly utilized procedure used for patients with chronic liver disease and resistant portal hypertension. Previous studies have explored the trends and short-term outcomes in TIPS procedures. This study aims to further compare short-term in-hospital outcomes of patients with chronic kidney disease when undergoing TIPS.
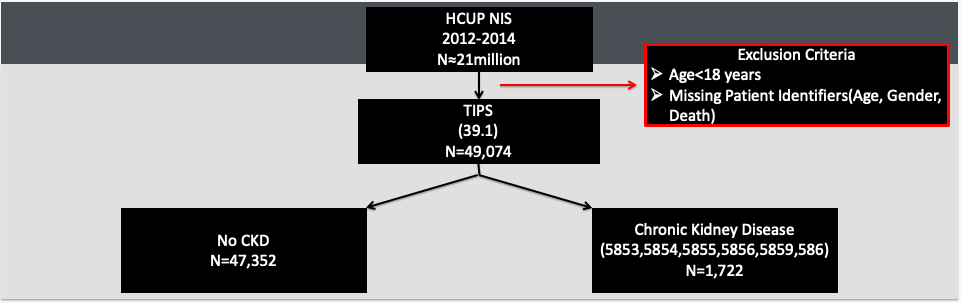
Methods: This retrospective cohort study utilized data from the Nationwide Inpatient Sample (NIS) to identify adult patients (18+) from 2012-2014 who underwent a TIPS procedure. ICD-9 codes identified patients with a history of chronic kidney disease. Patients missing important clinical identifiers (age, gender, death) were excluded. Data analyses assessed hospital length of stay (LOS), inpatient charges, and mortality rate.
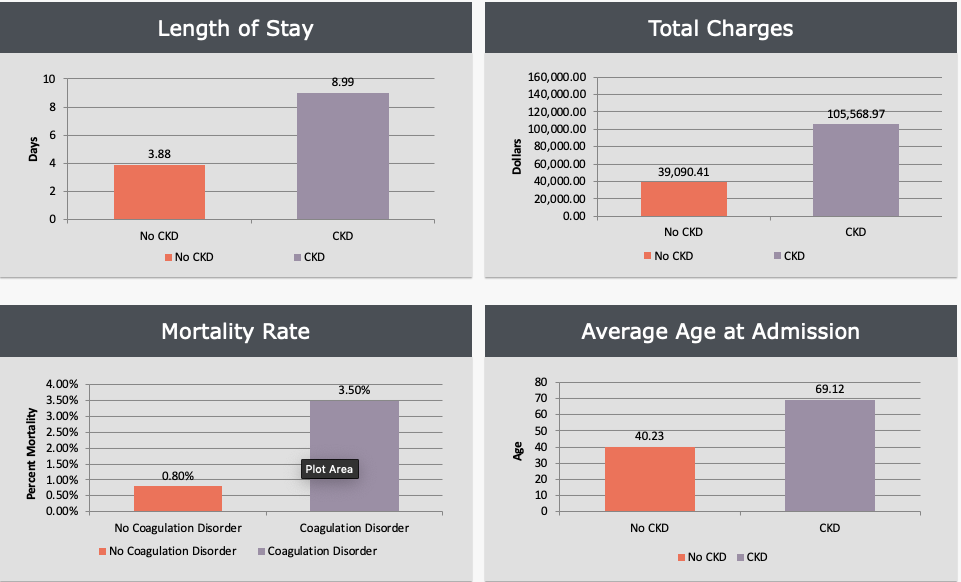
Results: Of the 47,352 patients identified to undergo a TIPS, 1,722 patients had a diagnosis of a chronic kidney disease. Patients without chronic kidney disease had a mean mortality rate of 0.8% and mean total hospital charges of $39,.090.21. Total hospital charges and mortality rate for patients with CKD were $105,568.97 (p ≤ 0.001) and 3.5% (p ≤ 0.001). LOS for patients without CKD was a mean of 3.88 days and patients with coagulation disorder was a mean of 8.99 (p ≤ 0.001) days.
Conclusions: Patients undergoing TIPS who are pre-disposed with chronic kidney disease suffer from longer LOS, increased total hospital charges and increased mortality rate. Optimization of treatment and management of prior diagnosed chronic kidney disease can provide avenues for lowering length of stay, total charges and mortality rate. Laboratory tests to screen and diagnose liver and renal failure, systemic infection, coagulopathy and to establish a Child-Pugh classification are all done prior to TIPS as it is imperative in managing hospital stay for these patients. It has been well-known that the kidney plays a major role in ammonia excretion post-TIPS procedure. While TIPS can be safely used in patients with CKD to treat chronic liver disease and portal hypertension, the risk of hepatic encephalopathy appears to be much higher in patients with abnormal renal function. Further analysis of the connection between CKD and hepatic encephalopathy can be looked at to further improve patient outcomes.