Background: Telemetry is frequently utilized in hospitalized patients for continuous cardiac monitoring but its inappropriate use has been linked to high healthcare costs, alarm fatigue, reduced mobility and extended emergency room boarding. A resident driven multimodal intervention including education on American Heart Association (AHA) 2017 guidelines was implemented to improve guideline-based telemetry use, telemetry duration and length of stay (LOS).
Methods: Our QI study was structured as Plan-Do-Study-Act (PDSA) cycle with two 2-month pre and post intervention data on telemetry usage and length of stay. We randomly collected data for 150 patients in each cohort with average case mix index (CMI) of 1.67 and 1.68 respectively indicating similar acuity. Interventions included resident/provider education, use of structured daily telemetry checklist, electronic health record (EHR) modifications to restrict telemetry order modifications to primary teams. Associations between telemetry days and LOS were evaluated using Pearson correlation and simple linear regression. Differences in means between pre- and post-intervention cohorts were assessed with Welch’s t-tests.
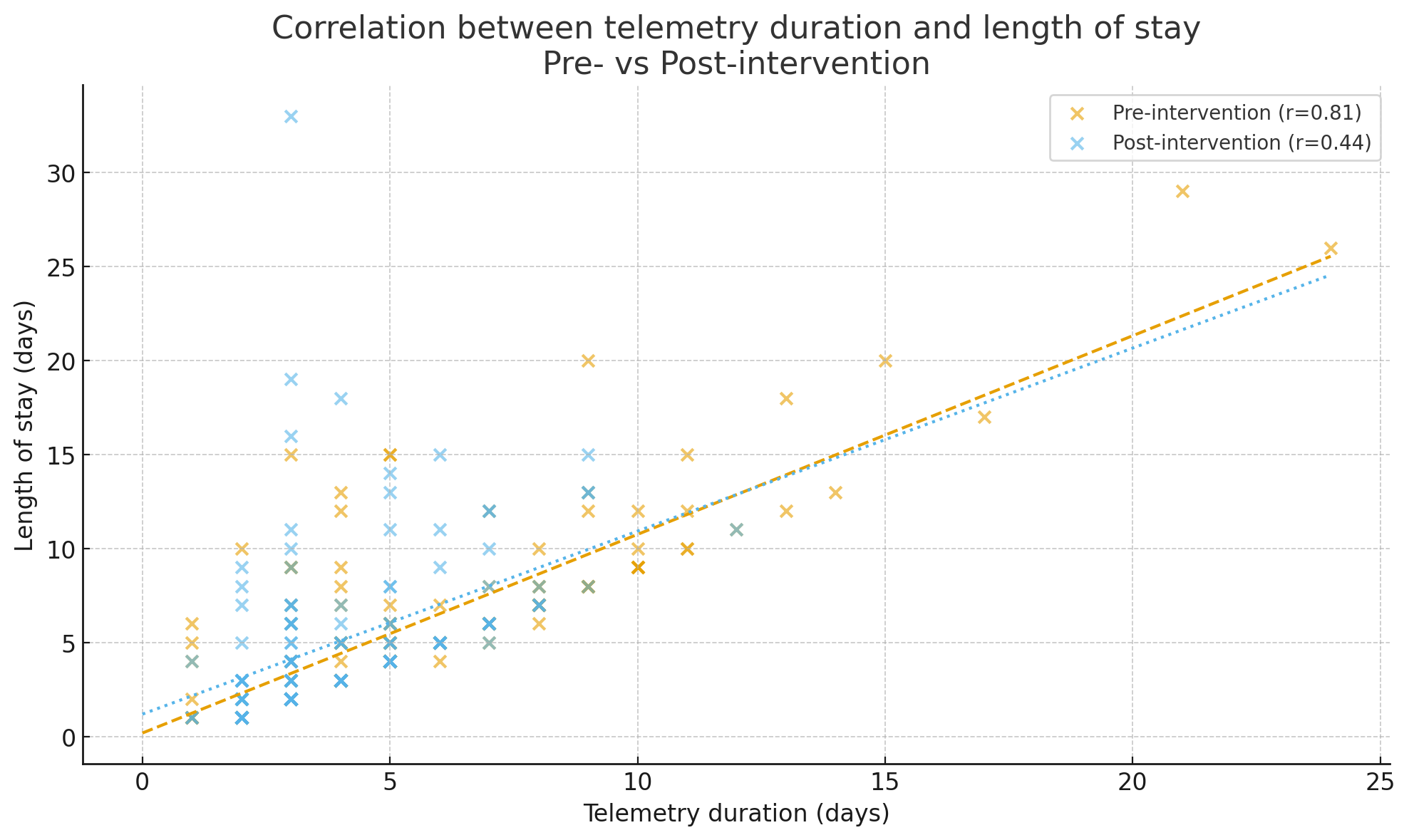
Results: Pre-intervention, the mean LOS was 6.1 days (SD 4.8) and mean telemetry duration 5.6 days (SD 3.7). Post intervention, significant improvement was observed in appropriate initial telemetry ordering from 72% to 90% (p< 0.001). Telemetry duration showed a strong positive correlation with LOS (r = 0.81, p < 0.001) and explained about 66% of LOS variability (R² ≈ 0.66). Post-intervention, mean LOS decreased to 5.1 days (SD 4.3) and mean telemetry duration decreased to 4.0 days (SD 2.0). Both telemetry duration and LOS were significantly lower post-intervention, with reduction in telemetry days (mean 1.7 days, P< 0.001) and reduction in LOS (mean 1.1 days, P=0.04). The correlation between telemetry days and LOS remained positive but was attenuated (r = 0.44, p < 0.001), with telemetry duration explaining about 20% of LOS variability (R² ≈ 0.20). The drop in correlation strength from 0.83 to 0.44 was also statistically significant (p < 0.001).
Conclusions: These findings suggest that a multipronged, resident-driven intervention combining education, structured checklist, and EHR modifications was associated with reduction in telemetry duration and LOS. Association of LOS with telemetry duration was stronger pre- intervention and reduced significantly post intervention. These findings indicate that appropriate telemetry utilization may reduce LOS and patient financial burden post-acute care hospitalization. Further analysis with multicenter larger patient data is warranted.