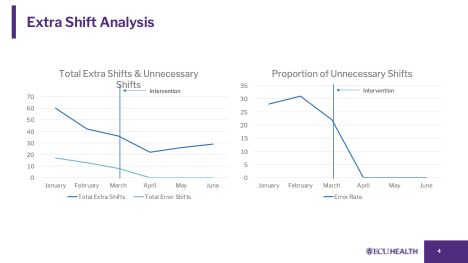
Background: Our group was compelled to pre-schedule backup rounders (16th and 17th providers) due to the rising and unpredictable hospital census. These shifts were often paid at premium rates, resulting in avoidable costs and inefficiencies, irrespective of the actual census, as perceived by the providers. From 2023 through early 2025, decisions to activate backup hospitalists were made using subjective judgment. This produced inconsistent staffing, unnecessary premium-rate call-ins. Between December 2024 and March 2025 alone, the hospitalist service generated 138 extra shifts, costing $345,000, including 38 shifts ($95,000) that did not meet objective need. Analysis of these periods showed high rates of False Positives (unnecessary call-ins), False Negatives (missed staffing needs), and growing census routinely over 350 patients, revealing the need for a structured, timely, and financially responsible staffing approach.
Purpose: To implement a standardized, transparent, census-based staffing model that activates additional providers only when objective thresholds are met, reducing avoidable premium shifts, while maintaining a patient-cap target of 18 per provider.
Description: We developed a transparent, census-based decision matrix used each morning to determine whether extra staffing is needed. Instead of scheduling fixed backup rounders, we created a voluntary “standby” pool of moonlighters who can opt in or withdraw freely. If census exceeds matrix thresholds, a standby provider is called in; if not, no additional coverage is activated.This model works in our environment because of a strong moonlighting pool and clear communication around how the matrix triggers are applied.
Conclusions: Before the intervention (Jan–Mar), the service used 138 extra shifts costing $345,000, including 38 avoidable shifts ($95,000). After implementation (Apr–Jun), extra shifts dropped to 77 with 0 avoidable, costing $192,500—a net savings of $152,500 in one quarter.A census-aligned standby model can substantially reduce unnecessary premium spending while preserving safe provider workloads. Ongoing adjustment is essential to adapt the model to seasonal and operational changes.