Background: Development of opiate use disorder and opiate overdose has been associated with prolonged opiate-days prescribed. Conventionally, opiate-days supplied has been calculated based on the discharge prescription signature (e.g., how a patient is supposed to take the medication) and the number of pills dispensed. It is not clear whether the number of days supplied reflects the actual opiate needs of the patient. We compared the days supplied using two metrics: one based on the discharge signature, and one adjusted for the amount of opiates required during the hospitalization.
Methods: We used the electronic health record to identify all patients hospitalized on the acute care medical service at a 600-bed tertiary care hospital from 2012-2018 who received opiates during hospitalization and were discharged on an opiate. We excluded patients likely to require extended opiate prescriptions (ICD9 or 10 code for cancer-related pain or sickle cell disease, or who were on hospice or followed by the palliative care service). For each hospital day, we ascertained the total amount of opiates administered that day, standardized to morphine milligram equivalents (MMEs). The number of opiate days supplied was first determined using the discharge prescription, based on the prescription signature and number of pills ordered. We then determined the number of opiate days supplied adjusted for the amount of opiates required by the patient during the last 24 hours of hospitalization. The difference in days supplied between the two measures was compared using t-tests.
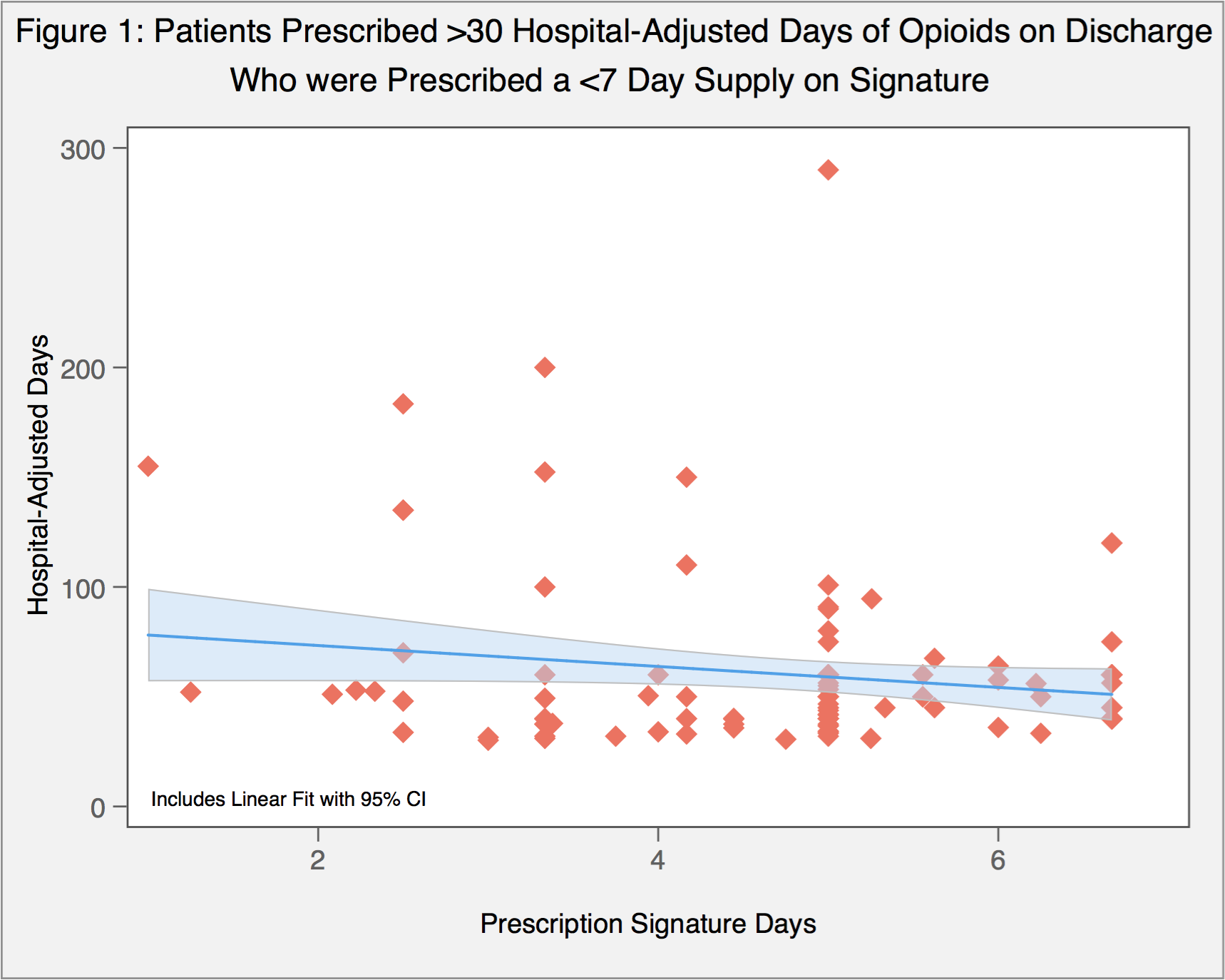
Results: We identified 6,902 patients with a baseline opiate prescription who were discharged on opiates, and 2,373 patients discharged on opiates without opiates on their admission medication list. The median MME per day of hospitalization was 57.7 mg [IQR 21.1 – 150.4], and 60 mg [IQR 24 ¬– 165] for the last 24 hours. Using the metric adjusting for the opiate needs on the last 24 hours of hospitalization resulted in a mean days supplied of opiates that was 3.6 days longer than when using a standard days supplied metric (11.9 vs 8.3 days, p<0.001). Patients with a baseline opioid prescription were prescribed a median of 10 days on discharge by prescription signature, and 14 days based on hospital requirements (p<0.001). Patients without a baseline opioid prescription were prescribed a median of 5 days on discharge by prescription signature, and 7.1 days based on hospital requirements (p<0.001). Of patients prescribed <7 days of opioids by discharge prescription signature, 126 patients (3.5%) received a >30 day prescription when adjusted for needs in the hospital (Figure 1) A total of 325 patients (8.0%) without a baseline prescription were discharged on opioids despite requiring no opioids in the 24 hours prior to discharge.
Conclusions: Days on a prescription signature and a calculation of days based on hospital need are two significantly different mechanisms to calculate discharge opioid-days. The amount of opiates supplied to patients at discharge may exceed their actual clinical needs, since the frequency with which a patient takes opiates at home after discharge may be better reflected by the adjusted days model.