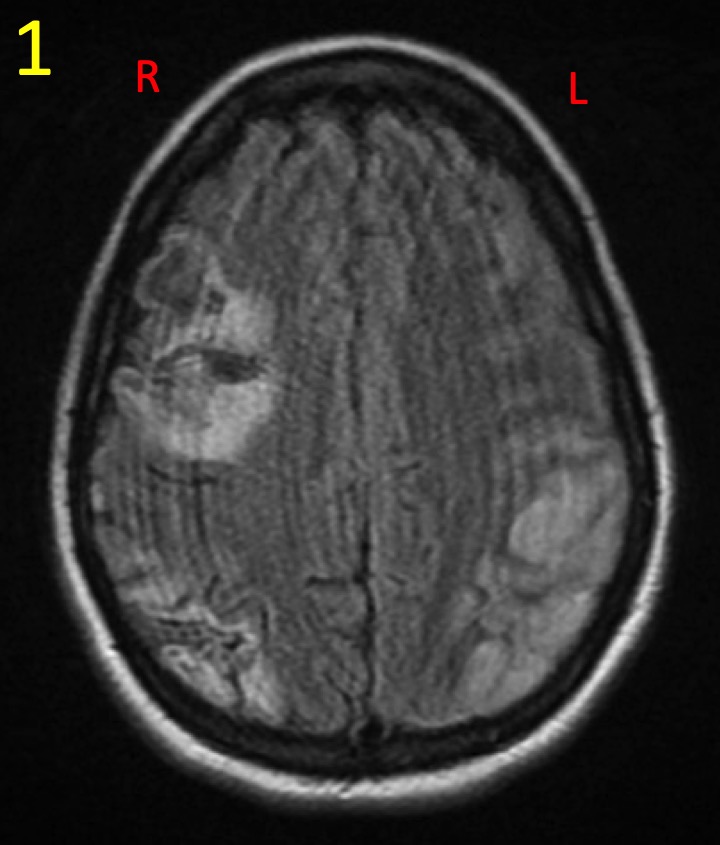
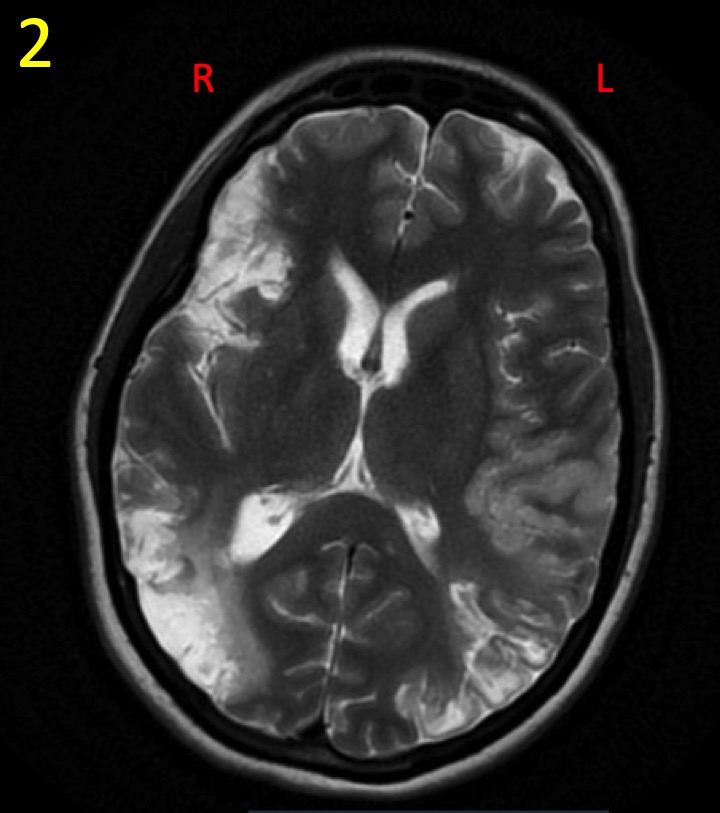
Case Presentation: A 42-year-old woman was admitted for recurrent multifocal cerebral infarction. She had five episodes of consecutive strokes involving different vascular territories over 8 months resulting in expressive aphasia, visual deficits, and extremity weakness. All laboratory and urine studies, including autoimmune and hypercoaguable workup were unremarkable. Treponema and HIV serologies were negative. Initial cerebral angiogram and lumbar puncture were unremarkable. Initial transthoracic echocardiogram (TTE) and transesophageal echocardiogram (TEE) demonstrated no evidence of patent foramen ovale (PFO) but it was technically difficult to visualize valves. An implantable loop recorder did not reveal arrhythmogenic activity. Antiplatelet and anticoagulation medications failed to prevent recurrence of strokes. Malignancy workup including CT scan of chest, abdomen, and pelvis was unremarkable. The etiology of recurrent strokes remained elusive. Subsequently, patient underwent further evaluation with left heart catheterization and intra-cardiac echocardiogram that ruled out PFO. A repeat TEE revealed small, highly mobile filamentous lesions attached to the atrial side of mitral leaflets and repeat cerebral angiogram showed multiple emboli in distal left middle cerebral artery. She was afebrile but reported night sweats and chills for several months. She lived in a rural area of Texas and had contact with livestock. The diagnosis of infective endocarditis was then entertained. Three sets of blood cultures and subcultures of the incubating blood cultures with buffered charcoal yeast extract (BCYE) were negative. Coxiella, Bartonella, Brucella, Chlamydia, and Coccidioides antibodies and Histoplasma antigen were negative. Legionella pneumophila type 1-6 IgG titer was highly reactive (1:512) but urinary Legionella serogroup 1 antigen was negative. Legionella endocarditis with embolic phenomena was suspected and levofloxacin was introduced. After initiation, patient showed a significant clinical improvement and did not develop further episodes of stroke. Repeat TEE after 6 weeks of treatment showed significantly smaller sized filamentous structures in the valve that nearly resolved at 6 months follow-up.
Discussion: Although our patient did not exhibit clinical stigmata for endocarditis such as those highlighted in modified Duke criteria and TEE did not clearly delineate valvular vegetation, clinical suspicion of infective endocarditis remained high in this circumstance. Legionella, a fastidious organism, is extremely difficult to grow on blood culture, which would explain the negative cultures, even with BCYE agar subcultures. Current guidelines recognize that serological testing may serve as a surrogate marker in the diagnosis of endocarditis caused by fastidious organisms. However, other than Coxiella, there is no specific titre cut-off for other pathogens to confirm the diagnosis. Serum PCR assays may be helpful but its role remains unclear. Our patient exhibited an improvement of clinical and radiological findings with resolution in recurrent strokes coinciding with levofloxacin therapy, making the diagnosis probable in this setting.
Conclusions: Legionella endocarditis is extremely rare. Embolic phenomenon in patients with Legionella native valve infective endocarditis has previously been reported in only one case. A high index of suspicion for culture-negative endocarditis is of paramount importance in the right clinical context.