Background: Capturing appropriate clinical documentation allows providers to best approach treating patients and can also be utilized for quality monitoring of outcomes within health systems. Mortality measures are used by the Centers for Medicare and Medicaid Services (CMS) for reimbursement and payment. (1) Observed mortality includes all deaths which occur in the hospital during a specific period, while expected mortality utilizes documentation to identify illness severity and predict a number of expected deaths. (2) Beyond demographic data, documentation of clinical problems directly impacts expected mortality. Observed mortality divided by expected mortality will deliver a mortality index- a metric by which hospitals and health systems can look at the quality of care they are providing, and CMS can utilize to support billing and reimbursement. However, without accurate documentation to create a precise expected mortality, there will be inaccurate mortality index. Review of mortality cases has been shown to improve documentation to better represent expected mortality. Several other specialties including critical care, surgery, neurology, and gynecology have utilized this method. (3,4,5)
Methods: A committee was convened including two oncology-hospitalists, one bone marrow transplant unit hospitalist, one oncologist, representatives from coding and clinical documentation improvement (CDI). Prior to each monthly meeting, mortality cases are randomly assigned to a physician to review looking for both clinical opportunities for intervention as well as documentation opportunities. Physicians are provided with a model mortality risk calculator as well as the Vizient variables that were used by coding. Physician review is captured by survey results which were submitted through Redcap. During monthly mortality committee meetings, physician identified documentation opportunities (PIDOs) are discussed as a group and if deemed appropriate, queries can be sent by CDI to the treating physician to capture additional variables. If PIDOs cannot be queried, CDI and coding explain what could have been documented to allow variable capture.
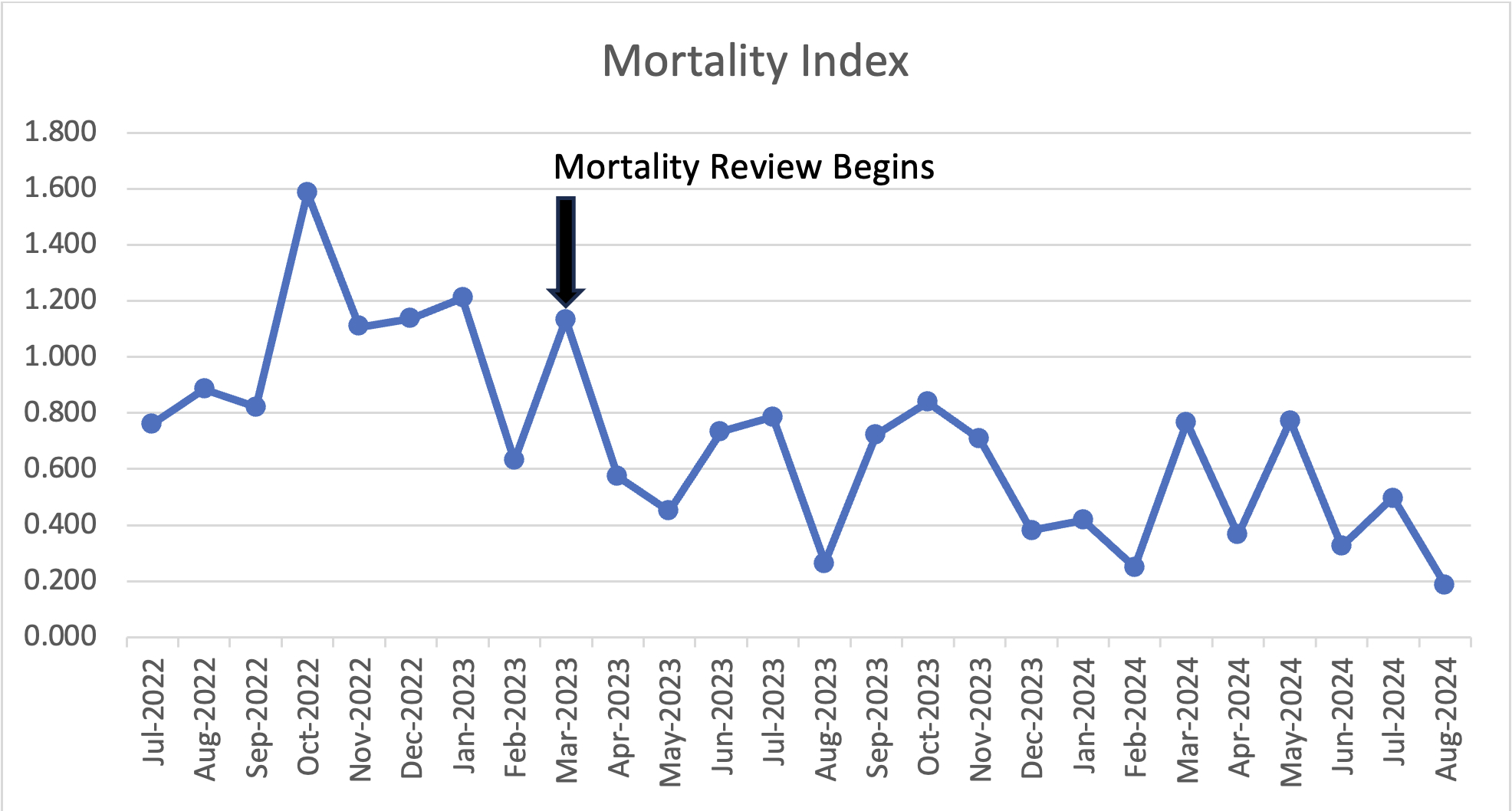
Results: Significant improvement was noted in mortality index on the hospitalist-run solid oncology service from the time mortality reviews began. Average mortality index prior to review was 1.030 which improved 0.523 post review. [figure 1]This improvement can be attributed to an increase in expected mortality from increased variable capture rather than a decrease in observed mortality as expected mortality increased from an average of 3.778 prior to review to an average of 5.05 after review. [figure 2]
Conclusions: Hospitalist and oncologist collaborative review of mortalities is an effective tool to improve mortality index for solid malignancy patients on a hospitalist run, solid oncology service. Improving expected mortality captures the complexity of patients cared for and the quality of care that is provided. This improvement in expected mortality and mortality index is thought to be in small part from queries sent to capture identified mortality variables, and in much larger part by education and awareness of opportunities that comes from direct interaction between physicians and members of CDI and coding. This interprofessional and interdisciplinary collaboration can be replicated at most institutions and showcases the important leadership role that hospitalists have in improving the quality of the care provided in a health system.