Background: Physician/Bedside Nurse (RN) communication is at the center of care delivery and patient experience for patients admitted to any Hospital Medicine service. While efficient communication within the healthcare team is the hallmark of high quality care, it is highly variable in terms of timing and quality. Inadequate communication between physicians and nurses, as perceived by patients, negatively impacts patient experience. We aimed to increase visibility of physician nurse communication for patients through bedside co-rounding on our Adult Hospitalist direct care service at University of California, San Francisco (UCSF). During the study period, the average daily patient census was about 87 on the UCSF Goldman service, the attending-only direct care service, through which more than 110 hospitalists rotate. There are many challenges to bedside co-rounding, some of them being dyssynchronous workflows, lack of geographic colocalization of patients, perception of co-rounding being time consuming, and variable rounding practices among hospitalists.Currently, there is no clear national benchmark regarding physician nurse co-rounding. Therefore, we have established our own internal benchmarks from data collected on the Goldman Hospitalist service at UCSF.
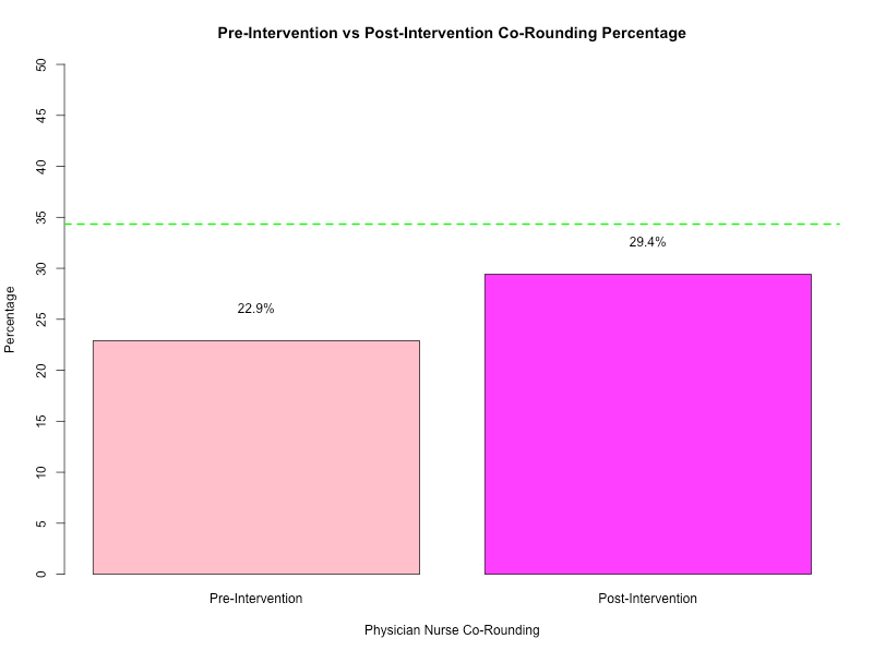
Purpose: We aimed for a 50% increase in bedside co-rounding from a baseline of 22.9% established in August 2023 to 34.4% by August 2024 for Goldman service patients with behavioral concerns through nurse-initiated invitations. To identify patient populations that would benefit most from physician-nurse co-rounding, we interviewed 11 hospital nurses and nurse managers. They highlighted three groups for whom bedside rounding would be most beneficial: patients with behavioral concerns, high-acuity or transitioning patients, and patients with complex pain management needs. Deferring to this experience of the frontline staff, we decided to focus on patients with behavioral concerns.
Description: During our gap analysis, we recognized that most co-rounding interventions so far have been physician driven with limited success. We propose that empowering bedside nurses to initiate co-rounding may be a powerful way to get both the physician and the nurse at the bedside.In our intervention, we began with an implementation period requesting nurses to message providers requesting bedside co-rounding for patients that have been identified to have behavioral concerns. We educated providers through flyers, nurse unit meetings, email reminders, and “real time” education on the nursing units.
Conclusions: Although we did not reach our goal of a 50% increase from baseline in bedside co-rounding for patients with behavioral concerns, we were able to achieve a significant improvement in physician nurse communication measured by bedside co-rounding rate. Pre-intervention data collected one year prior to our intervention demonstrated 22.9% co-rounding, while the data collected after incorporating our intervention displayed 29.4% co-rounding which is a 28% increase in co-rounding, demonstrating that our intervention reached the intended audience and trended towards reaching our goal. Some limitations included the limited study period and limited resources of this medical student quality improvement project. Future directions would involve expanding the intervention to encompass more patient populations by adoption of this practice as a prioritized quality improvement initiative driven by clinical service leadership.