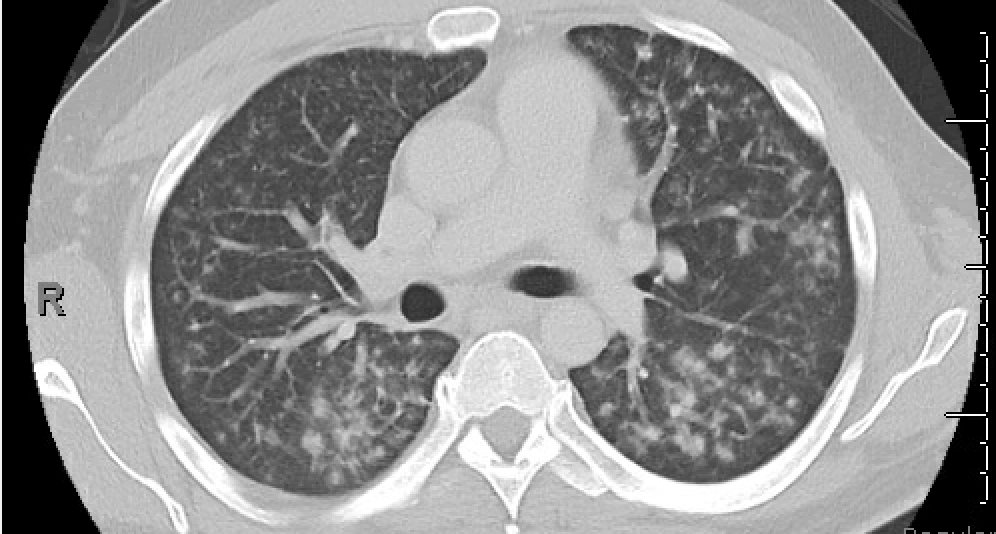
Case Presentation: A 43-year-old male presented to the emergency room with dry mouth and fever. The patient endorsed pain and dryness when eating solid foods. He noted 40 pounds of unintentional weight loss over 1 month. He had a 30 pack-year smoking history but reported no alcohol or illicit drug use. He did not take any medications at home. On arrival, he was febrile up to 102.6 F, tachycardic, and hypotensive. Physical exam revealed dry mucous membranes and partially edentulous but with submandibular lymphadenopathy and non-tender parotid gland swelling. Labs were remarkable for hemoglobin 9.0 g/dL, elevated erythrocyte sedimentation rate of 71 mm/hr and C reactive protein of 51 mg/L. White blood cell count was normal. A maxillofacial CT showed diffuse prominence of bilateral parotid glands with no evidence of salivary stones. CT Chest angiography showed groundglass opacities and solid nodules in the bilateral lung fields without overt mediastinal or hilar lymphadenopathy but was nondiagnostic for pulmonary embolism.He was started on broad spectrum antibiotics and a workup for underlying infectious and rheumatologic causes were pursued. SS-A, SS-B, rheumatoid factor, HIV, hepatitis C, blood cultures, histoplasma and Blastomyces antibodies, quantiFERON-TB gold testing and angiotensin converting enzyme level were all negative or within normal limits. Transesophageal echocardiogram did not show evidence of vegetation and blood cultures remained without growth. Fine needle aspiration of the parotid glands and bronchoalveolar lavage were unrevealing. The patient defervesced and was started on pilocarpine. Repeat CT chest showed worsening of the pulmonary infiltrates. Ultimately an endobronchial ultrasound with transbronchial biopsies showed non-caseating granulomas, indicating sarcoidosis. The patient was started on steroids with improvement.
Discussion: The lungs are the most commonly affected site for sarcoidosis. Exocrine gland involvement occurs in less than 6 percent of patient with sarcoidosis and is typically painless (1-2). Patients typically present with bilateral gland swelling and dry mouth (3). Nonspecific constitutional symptoms such as fever and weight loss can be seen with sarcoidosis. Fever is typically associated with Löfgren’s syndrome and Heerford-Waldenstrom syndrome (4). Our patient did not have skin involvement or hilar lymphadenopathy to suggest Lofgren’s syndrome nor anterior uveitis and facial nerve paralysis, characteristics of Heerford-Waldenstrom syndrome. Fever with diffuse lung nodules should also raise the question for infectious etiology (i.e tuberculosis and septic emboli). Only a few case reports had shown successful diagnosis of sarcoidosis with fine needle aspiration (5). As seen in this case, the initial presentation of sarcoidosis can be variable. Fine needle aspiration was negative for sarcoidosis in our case. Recognizing extrapulmonary sarcoidosis can be challenging but understanding the varied symptomatology of sarcoidosis and considering it on initial differential can lead to diagnosis and treatment. For our case with an atypical presentation, persistent workup and reexamining of presentation led to a firm, treatable diagnosis.
Conclusions: Exocrine glands involvement, although rare in sarcoidosis, should be in the differential when presented with pulmonary involvement (lung nodules, hilar lymphadenopathy, etc). Early treatment is important to prevent the progression of disease and disabling organ failure (ie lung scarring).