Background: Hospitalized patients and their families often face challenges in accessing and understanding developments in care plans, test results, and interdisciplinary decisions made during their stay. This knowledge gap causes anxiety, confusion, and missed opportunities for shared decision-making. Enhanced interdisciplinary communication and transparency with patients positively impacts patient satisfaction, readmission rates, patient safety and adherence to medical recommendations (1,2). The use of family-centered communication programs for hospitalized patients has been associated with medical error reduction and improved patient/family experience (3). Traditional bedside communication is often insufficient, however, as acutely ill patients are not always able to engage in their care plan and family members are not often available during rounds. In UC San Diego Division of Hospital Medicine, we hold daily interdisciplinary bedside rounds with patients and their families to discuss the care plan; participation in these rounds has been associated with improved patient engagement, satisfaction, and care quality metrics. However, access to this discussion is limited to those present and able to participate on rounds, narrowing the reach of this intervention.
Purpose: Our goal was to design and implement an electronic patient deliverable to bridge the communication gap between inpatient healthcare providers, hospitalized patients, and their families. We aimed to create a tool that captures key information discussed during daily interdisciplinary bedside rounds, making the care plan accessible to patients and their families via a secure patient portal, to be reviewed at their convenience.
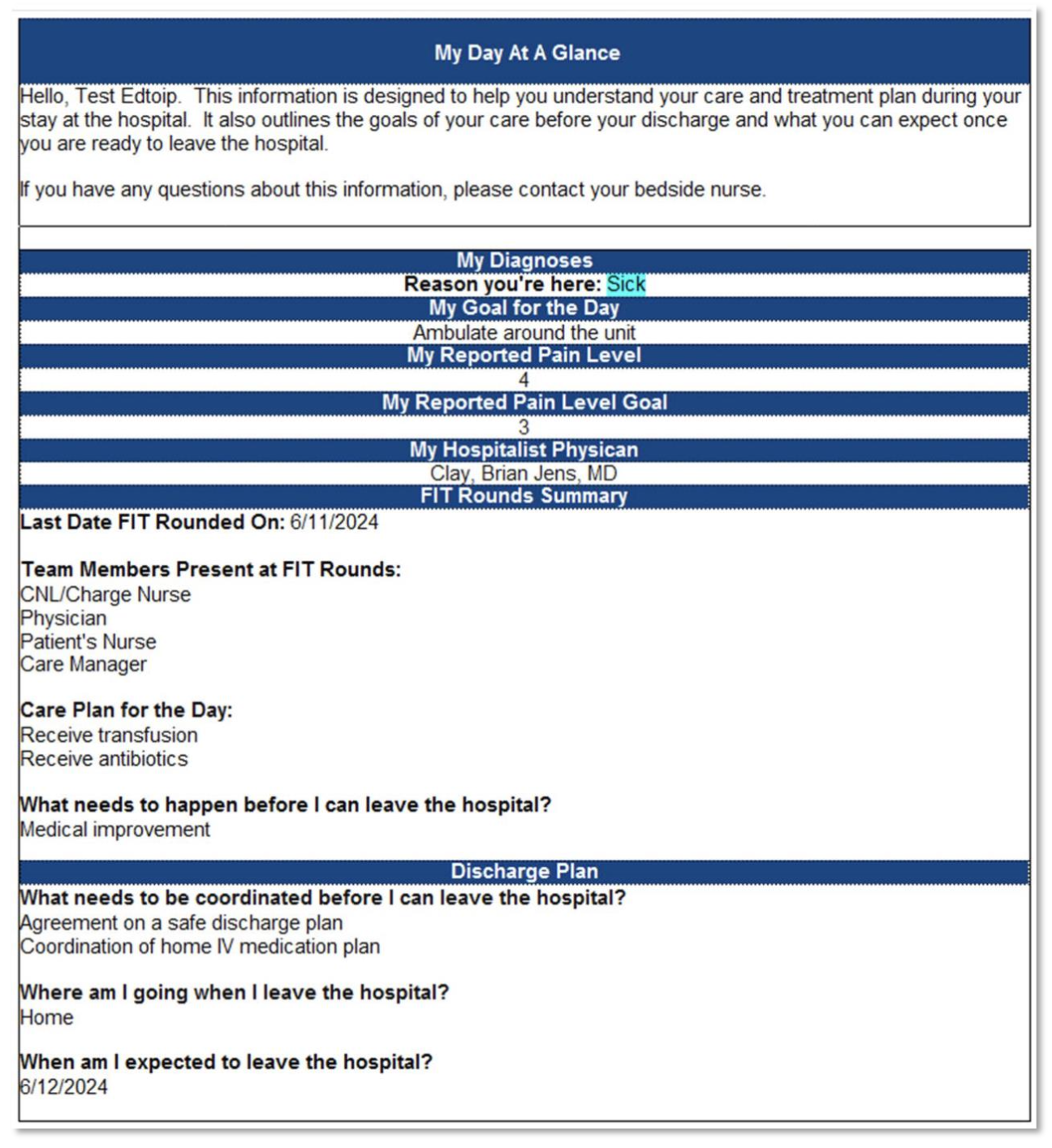
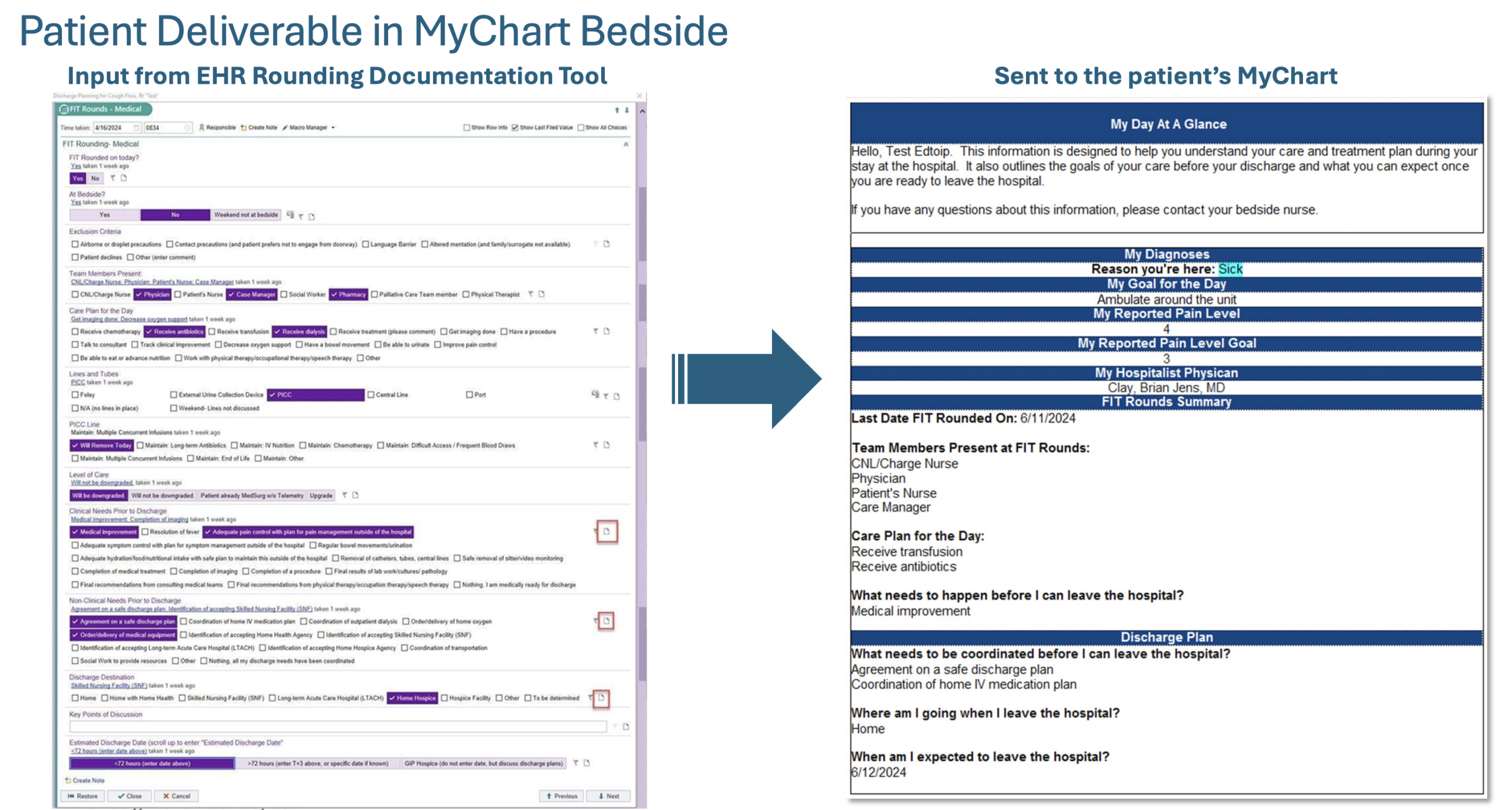
Description: We formed a multidisciplinary work group with representation from hospital medicine, nursing, care management, information technology, and patient experience to design a standardized template (Figure 1) within the secure patient portal to deliver daily care plan summaries to patients. To reduce redundancy, we leveraged data collected in real-time during our interdisciplinary rounds via an electronic health record documentation tool (Figure 2) to populate the patient deliverable. We updated our documentation tool to include click-boxes with patient-facing language so that data could be pulled directly into the deliverable. This delivered report summarizes all critical aspects of the hospitalized patient’s care journey – reason for admission, care plan for the day, remaining clinical milestones, and key elements of discharge planning. This information updates in real-time and can be accessed by patients and authorized family members at any time via the secure portal. Currently, utilization is limited to English-speaking patients with reliable access to the electronic patient portal, highlighting equity gaps to be addressed in its next iteration. Opportunities for expansion include automated notifications for care plan updates, multilingual resources, and digital record access education.
Conclusions: An electronic patient deliverable that summarizes the inpatient multidisciplinary care plan enhances patient-provider communication. By providing hospitalized patients and their families access to real-time updates on care plans and hospital progress, we can better engage in shared decision making and facilitate safe discharge planning. This tool offers a meaningful step toward patient empowerment and improved healthcare transparency.