
Background: Hospital Medicine (HM) and Emergency Medicine (EM) teams across 15 hospitals in the Jefferson Health–Lehigh Valley Region identified inefficiencies in the admission process that delayed initiation of inpatient care. Common barriers included disagreements regarding appropriate disposition such as ICU versus medical wards, or Hospital Medicine versus other specialty services. These delays hindered timely treatment and contributed to frustration among both patients and clinicians.
Purpose: The primary aim was to optimize patient safety and throughput efficiency by redesigning admission workflows to streamline order entry, reduce delays, expedite initiation of inpatient care, and improve satisfaction among multidisciplinary care teams.
Description: As a first step to optimize the admission process, EM and HM teams were surveyed regarding common diagnoses and services that contributed to delays in disposition decisions. Criteria for ICU‑level care or specialty service admissions were established based on team feedback and in collaboration with relevant subspecialists. Standardized communication was implemented through secure messaging to initiate admission requests. EM clinicians confirmed patient agreement, site appropriateness, and absence of ICU or specialty service criteria, documented a draft ED course in Epic, and sent a secure SBAR‑formatted message to HM triage with chart linkage and callback information. Most admissions proceeded via an expedited pathway in which the triage hospitalist placed admission orders immediately upon acknowledgment of the EM secure message. HM triage clinicians reviewed referrals within 30 minutes, communicated admission status and level of care, and placed bed requests or directed EM to place streamlined admission orders within 15 minutes. If HM did not place orders within that timeframe, EM clinicians were empowered to proceed. Exclusion criteria were established for patients requiring in‑person evaluation prior to admission, including elevated Modified Early Warning Score (MEWS), high Epic Inpatient Deterioration Index (IDI) scores, altered mental status, respiratory insufficiency, intoxication, or need for step‑down monitoring. Conversely, patients with low‑acuity diagnoses or potentially preventable readmissions were redirected to outpatient care when resources allowed. Once accepted, HM triage handed off to the admitting hospitalist via secure messaging. Admitting clinicians placed admission orders within 30 minutes and completed full admissions within 2 hours, using telemedicine or in‑person evaluation as appropriate. In‑person exams were required if the patient remained at the same site. For ED boarders, the ED Boarder Algorithm guided ongoing co‑management.
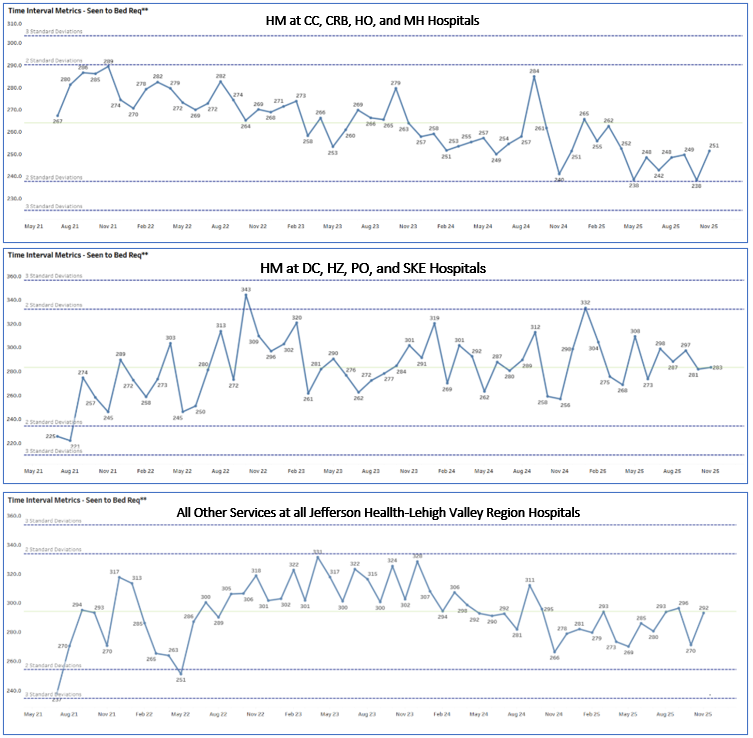
Conclusions: The redesigned admission process eliminated significant delays between admission decisions and order placement, reducing frustration for both patients and clinicians. Implementation decreased “seen‑to‑bed request” times defined as the interval from ED clinicians assigning themselves to a patient chart to admission order placement compared with hospitals not using the process and with other service line admissions. Through multidisciplinary collaboration, structured admission criteria, and effective communication via secure messaging, Jefferson Health–Lehigh Valley successfully streamlined workflows, improved clinician satisfaction, and enhanced efficiency in patient care delivery.
.png)