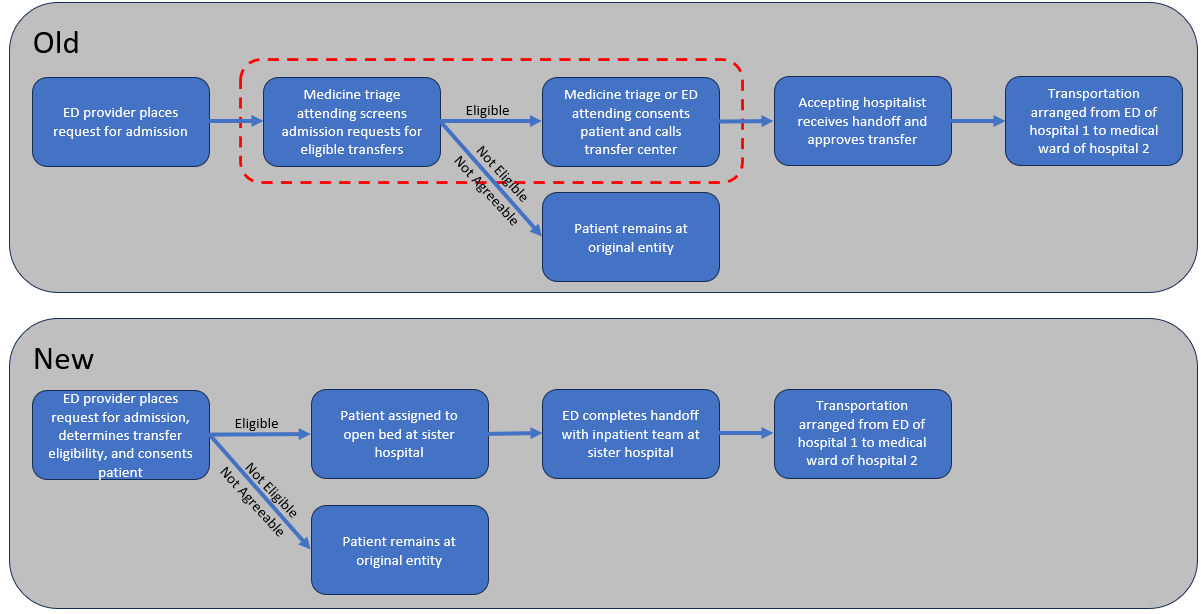
Background: Emergency Department (ED) boarding is a widely recognized problem(1). Over two decades of published research has demonstrated a link between ED boarding and an increase in patient mortality(2), as well as decreased patient, family and staff satisfaction(3). A common solution is a capacity command center, which centralizes the various functions of patient flow, including movement between hospitals in the same health system. In this modern healthcare environment, facilitating transfers between hospitals is integral to assigning the right patient the right bed at the right time, and has been used to reduce ED boarding(4). In our health system there are three hospitals co-located in the same city, with an uneven patient volume distribution: two of the hospitals have greater ED boarding than the third. Efforts had been made to transfer ED patients requiring admission directly to the wards of the hospital with greatest capacity. Traditionally, the identification, consent, and handoff steps were completed by the hospitalist triage attending in the ED. However, the siloed nature of capacity management at the three hospitals made this process challenging – transparency around bed availability was limited, and even after a patient was identified and consented, the triage attending was required to submit a transfer request through respective capacity centers to complete the process (Fig. 1). This inefficient process was identified as a factor limiting transfer volume.
Purpose: The purpose of this project was to decrease emergency department boarding at a multi-hospital academic health system.
Description: In this project, we integrated the capacity management functions for the hospital medicine services of all three hospitals into one department, in order to facilitate interfacility transfers between EDs and hospital wards. We created a new workflow wherein the ED physician placing an admission request checks a box to identify whether a patient is agreeable and clinically eligible for transfer (based on agreed-upon clinical criteria), and these patients are queued within the electronic health record for assignment by bed managers to any open medicine bed in the three hospitals. Once a bed is identified, the admission proceeds nearly identically to that of an admission staying in the native hospital. This new system streamlines the transfer process, reduces the number of handoffs, and functions 24 hours a day.
Conclusions: The new integrated system appears to be effective at increasing transfer volume and reducing boarding. In the 3 months preceding the start of the new system, 89 patients were transferred from the EDs of hospitals 1 and 2 to the medical wards of hospital 3. In the first 3 months of the integrated capacity system, there were 195 such transfers. Notably, the number of transfers was limited by bed availability at hospital 3, as an additional 686 patients were agreeable but did not transfer. For the first three months of the new system, the median boarding time for medicine admissions decreased by 1.7 hours and 1.2 hours at hospitals 1 and 2, respectively. For patients who elected to move to hospital 3, the average time from admission request to inpatient bed arrival was under 4 hours, meeting the Joint Commission Guidelines. It is anticipated that the integrated bed management system will be expanded to additional service lines in the near future.