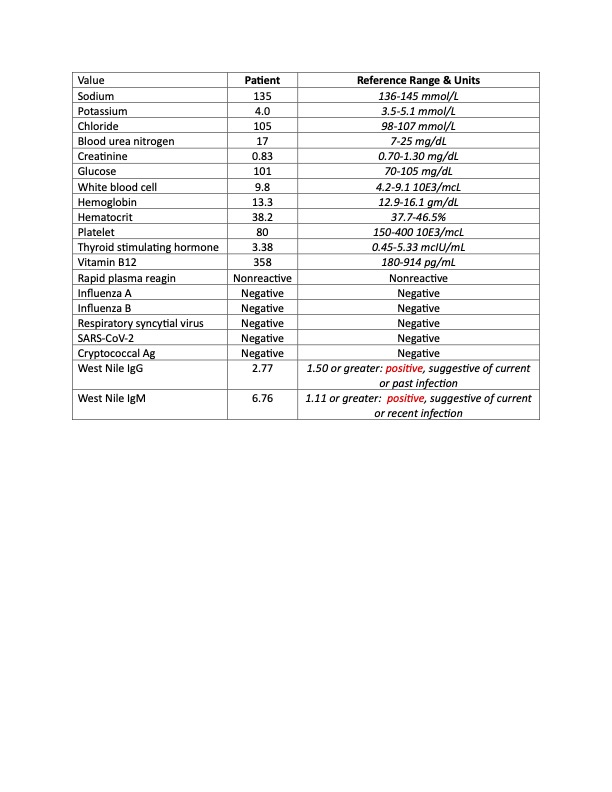
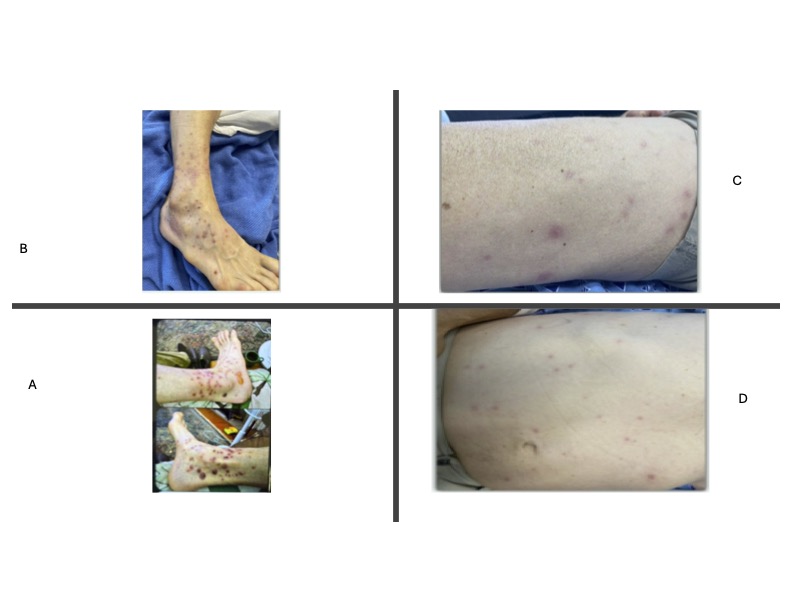
Case Presentation: A 68-year-old man was presented to the emergency department with headache, confusion, sweats, body aches, and nonproductive cough. He had recently returned from a solo hiking trip in the woods where he not only swam in a lake but also was exposed to poisonous plants and bitten by mosquitoes and other insects. The patient’s sister, a radiologist, expressed concern about possible parasitic infections. His past medical history was significant for hepatitis C that was previously treated but complicated by cirrhosis.On initial examination, temperature was 37.4, blood pressure 88/59, heart rate 77, respiratory rate 16, and oxygen saturation of 94% on room air. Physical exam was notable for dry mucous membranes and a macular rash on his legs and torso (photo). Pertinent laboratory results included hyponatremia, leukocytosis, and thrombocytopenia. Given initial concern for sepsis, patient was started on empiric antibiotic therapy. The patient declined lumbar puncture (LP), making definitive testing for central nervous system (CNS) infections more challenging.His headache resolved after IV fluid administration. Antibiotics were discontinued after 24 hours as no obvious source of infection was identified. However, given his exposure history and clinical presentation, serologic testing for West Nile virus (WNV) was ordered. Over the next 48 hours, the patient improved clinically, becoming symptom-free. He was discharged home with instructions to use insect repellent when outdoors. During a follow-up telephone interview one week after discharge, the patient reported feeling well with no residual symptoms. His WNV serology confirmed acute infection (Table 1).
Discussion: WNV infection has been reported in the Northeastern United States. WNV is a single-stranded RNA virus transmitted through mosquito bites. Most infected individuals remain asymptomatic, while approximately 20% develop mild symptoms such as fever, headache, malaise, and rash. Severe cases mostly occur in patients with comorbidities and >60 years of age, presenting with neurological involvement including encephalitis or meningitis. The mortality rate in patients with CNS involvement is around 10%. Treatment is supportive, focusing on symptom management. Recovery is usually complete in mild cases, though severe cases may take weeks to months. Post-infection immunity is believed to be lifelong. No vaccine is available to prevent this disease but avoiding outdoor activities in areas where WNV is prevalent and using insect repellent containing DEET when necessary is important to avoid mosquito-borne infection such as WNV.
Conclusions: WNV cases will continue to occur across US and severe neuroinvasive cases will require hospitalization. Hospitalists should include WNV in their differential diagnosis and incorporate serological testing if CSF is not readily available.