Background:
The Centers for Medicare & Medicaid Services (CMS) have sought to reduce readmissions through penalties applied to hospitals with readmission rates that are higher than expected, as calculated from models that use patient-level administrative data to account for case mix. Similar approaches are used to determine expected morality rates. Currently, CMS disseminates hospital-level adjusted 30-day mortality rates for Medicare fee-for-service beneficiaries with discharge diagnoses of stroke, heart failure, myocardial infarction (MI), chronic obstructive pulmonary disease (COPD) and pneumonia, and principal procedure of coronary artery bypass grafting (CABG). We sought to examine the relationship between hospital-wide adjusted 30 day readmissions and condition-specific death rates across the acute care hospitals in the United States.
Methods: We used data published by CMS from July 1, 2011 through June 30, 2014. In total, 4452 acute care facilities were included based on having hospital-wide readmission rates, but not all facilities contributed data for each mortality measure. We excluded from analysis on a measure-by-measure basis those facilities for which outcomes were absent; we did not impute missing outcome measures since low volume of a given condition was the main reason for not reporting a measure. For each mortality metric, we constructed a logistic regression model to quantify the odds of performing in the lowest (best) mortality tertile as a function of readmission tertile. To account for patient volumes, we included in each model the number of eligible patients at each hospital with the specified condition.
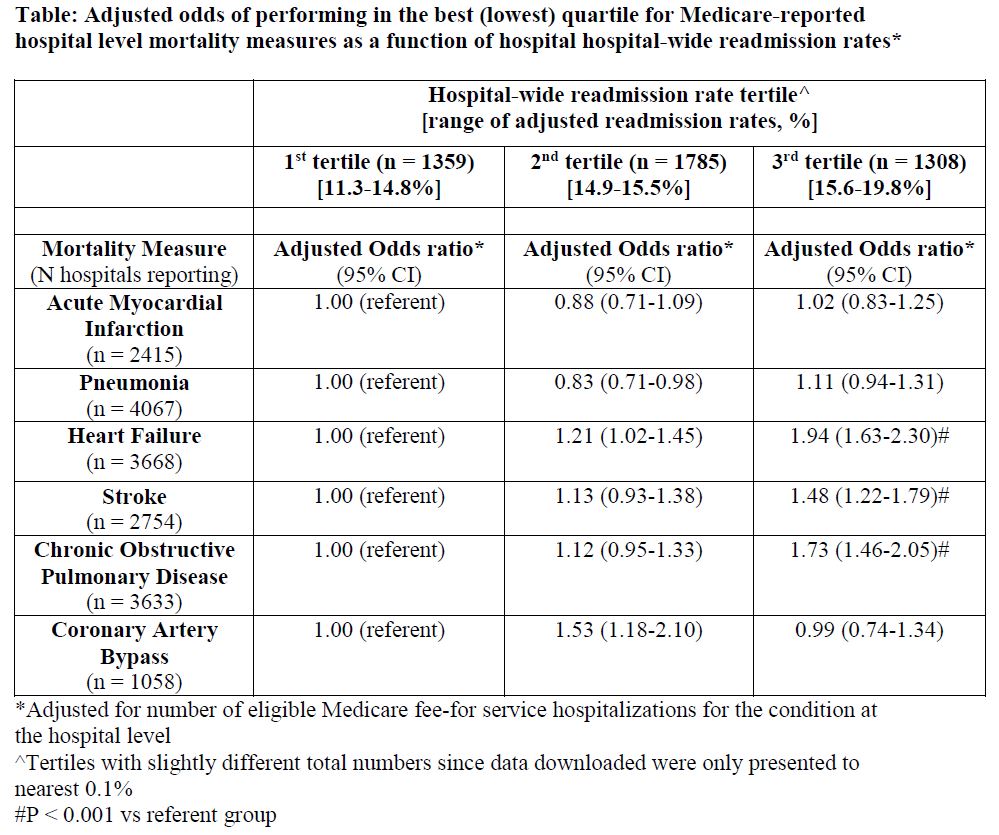
Results: Hospitals in the highest readmission rate tertile were more likely to perform in the lowest (best) mortality tertile for 3 of the 6 mortality measures: heart failure, COPD, and stroke (P < 0.001 for all). For MI, CABG and pneumonia, there was no significant association between high readmission rates and low mortality. (Table)
Conclusions:
We found that higher hospital-wide readmission rates were associated with lower mortality at the hospital level for 3 of the 6 mortality measures we examined. The findings for heart failure parallel the findings of Krumholz and colleagues who examined 3 of these 6 measures (MI, pneumonia and heart failure) in relation to readmissions for these specific populations. These prior data, however, did not include the three more recently reported mortality measures (COPD, stroke, and CABG) and did not use hospital-wide readmissions. While it is certainly possible that efforts to keep patients out of the hospital might, in some instances, place patients at risk by delaying necessary acute care, it is also possible that unmeasured variables, particularly access to hospice and palliative care services which might facilitate “good” deaths could be associated with both reduced readmissions and higher death rates. Nevertheless, we suggest that while hospital-level readmission rates are potentially valuable utilization metrics that can be targeted for cost containment, caution is warranted in viewing hospital-wide readmissions as a quality metric (as in the star rating system), until the associations we describe are better explained using patient level data and more robust adjustment than is possible with these publically available data.