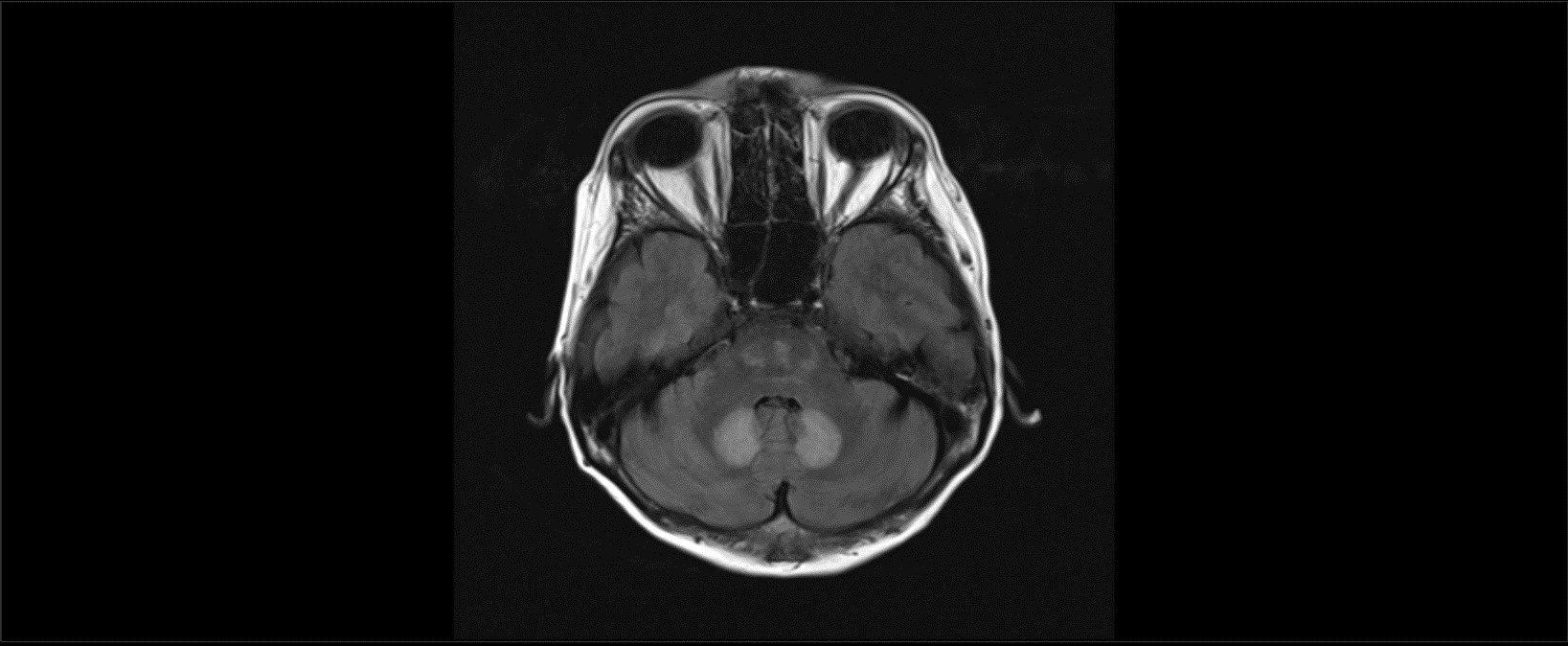
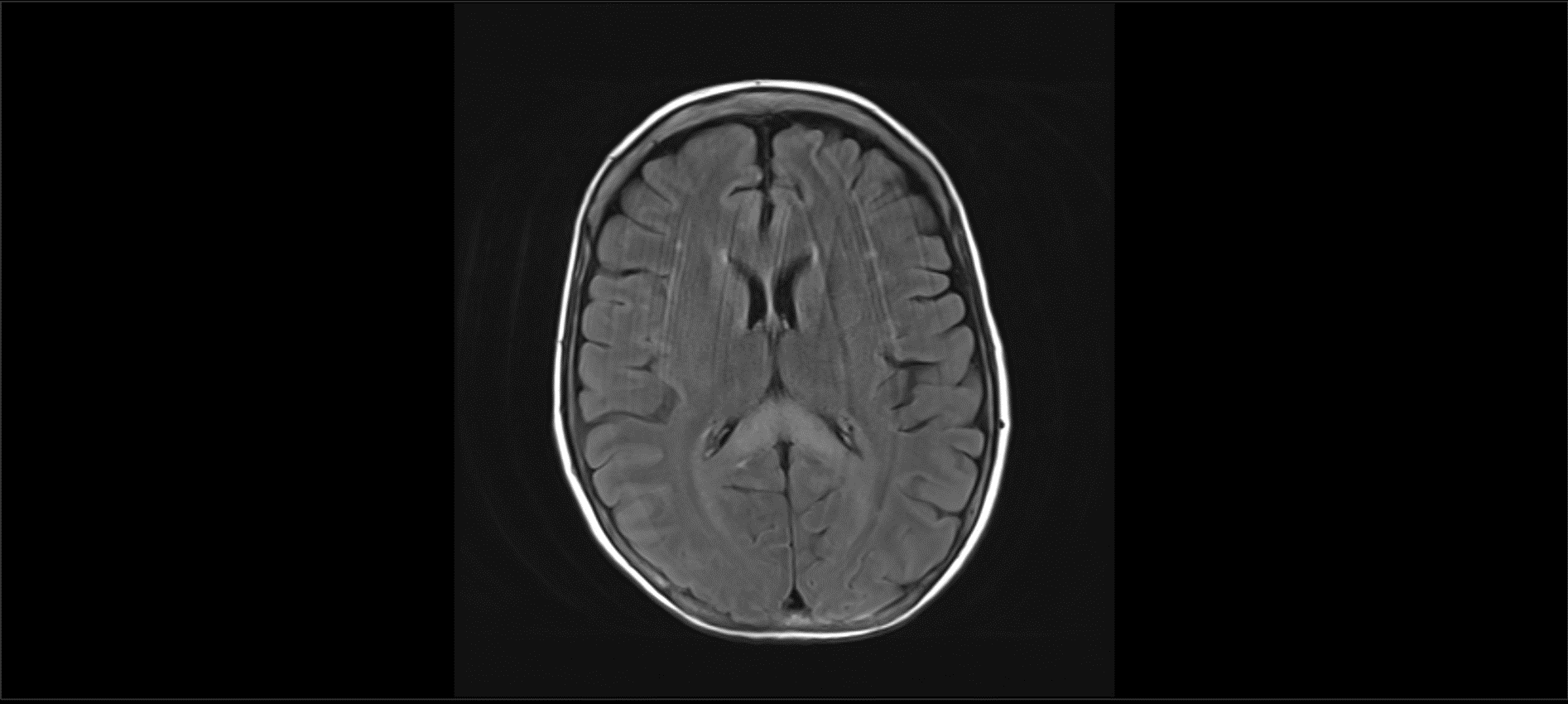
Case Presentation: We report a case of a 44 year old female with a history of hepatitis C and alcoholic cirrhosis, abstinent from alcohol for about two years, who presented from a nursing facility with few weeks of confusion and bilateral lower extremity weakness and imbalance. Her family reported that she was oriented, communicative and ambulating without assistance a week prior to admission. She was compliant with her lactulose but mentioned that her appetite had decreased since initiation of lactulose. She was started on oral metronidazole 500mg every 8 hours with the onset of her confusion and family reported worsening in her weakness and imbalance with this change mentioned above. On exam, she was weak in her bilateral hip flexors with 4/5 strength on testing. Her finger to nose testing was preserved but she was sluggish on heel to shin testing bilaterally suggesting truncal ataxia. Pertinent labs findings were as follows: sodium 134 mmol/L, creatinine 0.56 mg/dl, WBC 8200. Her UA and other infectious workup was negative. Her ammonia was minimally elevated at 44 umol/L (normal: 11-35 umol/L). MRI brain with and without contrast revealed regions of T2/FLAIR signal hyper intensity located in the dentate nuclei, splenium of corpus callosum, and in the pons. This pattern of signal abnormality, specifically involving the dentate nuclei bilaterally is typical for metronidazole-induced encephalopathy (MEI) (Image 1A). The involvement of the splenium of the corpus callosum also suggest likely component of Marchiafava-Bignami (MB), commonly seen with malnutrition due to deficiency in B vitamins (Image 2A). Metronidazole also causes reversible peripheral neuropathy worsening his patient’s unsteadiness and gait imbalance.
Discussion: MIE is a rare toxic encephalopathy with characteristic T2 hyper intense lesions of the bilateral dentate nuclei leading to predominantly cerebellar findings on exam. The mechanism of metronidazole toxicity has not been elucidated, and the apparent preferential involvement of the dentate nucleus remains puzzling. It can be differentiated from Wernicke’s encephalopathy, which presents similarly, but has MRI findings of bilateral symmetric T2 hyper intense lesions in the periventricular regions of the mammillary body, medial thalamus, floors of the third and fourth ventricles, periaqueductal gray matter, and midbrain tectum. Additionally, we cannot rule out Marchiafava-Bignami especially given involvement of the entire corpus callosum and clinical history suggesting malnutrition and alcoholism. Our patient did improve with discontinuation of metronidazole and she did report improvement in her strength at her post discharge follow up suggesting a large component of acute metronidazole encephalopathy and neuropathy
Conclusions: There are a few reported cases describing these imaging findings of metronidazole toxicity in literature. We present this case to raise awareness of an adverse yet reversible side effect of a commonly prescribed medication by hospitalists.