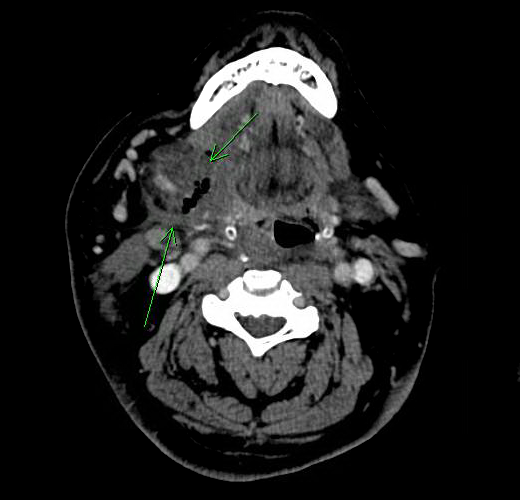
Case Presentation: A 58-year-old male with hypertension, morbid obesity and obstructive sleep apnea (OSA) was shifted to MICU for monitoring of his respiratory status following elective vitrectomy under general anesthesia. He was managed with non-invasive ventilation (NIV) for OSA overnight. Next day he developed an acute onset, right-sided painless neck swelling without associated dysphagia, odynophagia or stridor. Physical examination was remarkable for overlying erythema, mild desquamation without fluctuance or crepitus. Floor of the mouth was tender to palpation. He was afebrile with normal white count. CT scan showed asymmetric enlargement and edema of the right submandibular gland with multiple foci of gas within the gland and surrounding tissues concerning for necrotising fascitis. Empiric antibiotic therapy with vancomycin, piperacillin-tazobactam and clindamycin was started. His clinical course was stable without any features of systemic toxicity. Blood cultures showed no growth after 48 hours so antibiotic therapy was deescalated. A clinical diagnosis of traumatic intubation followed by extravasation of air into the soft tissues as a result of positive pressure non-invasive ventilation was made. Patient was observed for 48 hours with resolution of swelling and erythema.
Discussion: Necrotizing fasciitis (NF) is a microbial infection involving soft tissue, causing disseminated necrosis and eventual systemic toxicity leading to death. Due to its associated high morbidity and mortality, NF should preferably be misdiagnosed rather than being a missed diagnosis. Our patient had an acute onset of right sided swelling with imaging evidence of soft tissue gas, raising concerns for necrotizing fasciitis. The absence of tenderness, fever, leukocytosis and systemic symptoms suggested otherwise. Occult trauma from intubation or irritation form endotracheal tube, complicated by forceful air entry into the interstitium and submandibular space from NIV lead to the described clinical picture.
Conclusions: Acute traumatic perforation accounts for 6% of airway management complications with most frequent sites being the larynx (33%), pharynx (19%), and esophagus (18%). Aggressive as it is, NF is an under recognized consequence of traumatic airway management. It can result from break in the integrity of soft tissues following surgery or instrumentation. A rather benign condition following traumatic intubation is described here, that can masquerade as NF. Therefore, imaging evidence of gas in the soft tissue needs to be managed in the right clinical context.