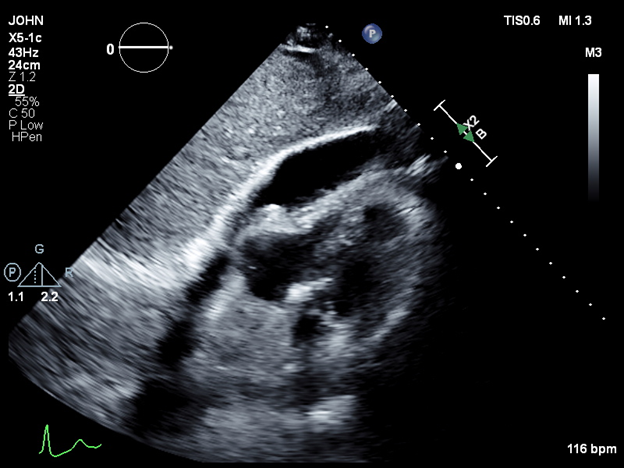
Case Presentation: We present the case of a 70-year-old male with a medical history of atrial fibrillation, hypertension, hyperlipidemia, and chronic obstructive pulmonary disease (COPD), admitted for elective radiofrequency ablation for atrial fibrillation. In the immediate postoperative period, the patient became hypotensive, with a blood pressure of 60/40 mmHg, and developed tachycardia, with a heart rate of 118 bpm. A bedside echocardiogram revealed a pericardial effusion with tamponade physiology. The patient was emergently transferred to the intensive care unit, where he was intubated and started on norepinephrine. An arterial line and central venous catheter were placed. Echocardiographic findings confirmed a large pericardial effusion, and a pericardial window was performed, draining 300 mL of bloody fluid. The patient also presented with bilateral pneumothoraces, and esophageal perforation was suspected due to the presence of mediastinal air. Bilateral thoracostomy tubes were inserted. However, subsequent endoscopy ruled out esophageal perforation. After clinical stabilization, the patient was successfully extubated and transferred to the internal medicine service. Both thoracostomy tubes were removed, and the patient was safely discharged home.
Discussion: Cardiac tamponade is a rare but potentially life-threatening complication following cardiac ablation. Studies have identified several risk factors, including female gender, hypertension, and older age, which increase the likelihood of cardiac tamponade in patients undergoing this procedure [1]. While cardiac ablation has become a mainstay treatment for atrial fibrillation, with its ability to restore sinus rhythm and reduce long-term stroke risk, rare complications such as tamponade can occur in approximately 0.7% of cases, warranting further investigation to identify at-risk populations and mitigate harm [2]. This case highlights the importance of rapid recognition and management of life-threatening complications following atrial fibrillation ablation. Cardiac tamponade, while rare, can have a catastrophic impact if not promptly addressed. The immediate use of bedside echocardiography, followed by hemodynamic stabilization with intravenous fluids, vasopressors, and positive pressure ventilation, played a critical role in this patient’s survival [3]. Developing standardized protocols for the prompt identification and management of such emergencies in cardiac care can significantly improve outcomes in hospital settings, ensuring that patients receive timely interventions.
Conclusions: Cardiac tamponade remains a significant but rare complication of atrial fibrillation ablation, underscoring the importance of vigilance during the postoperative period. This case serves as a reminder of the value of early diagnosis and intervention in preventing severe outcomes. Continued research into identifying at-risk populations and refining procedural techniques will be essential to reducing the incidence of this complication and improving overall patient safety.