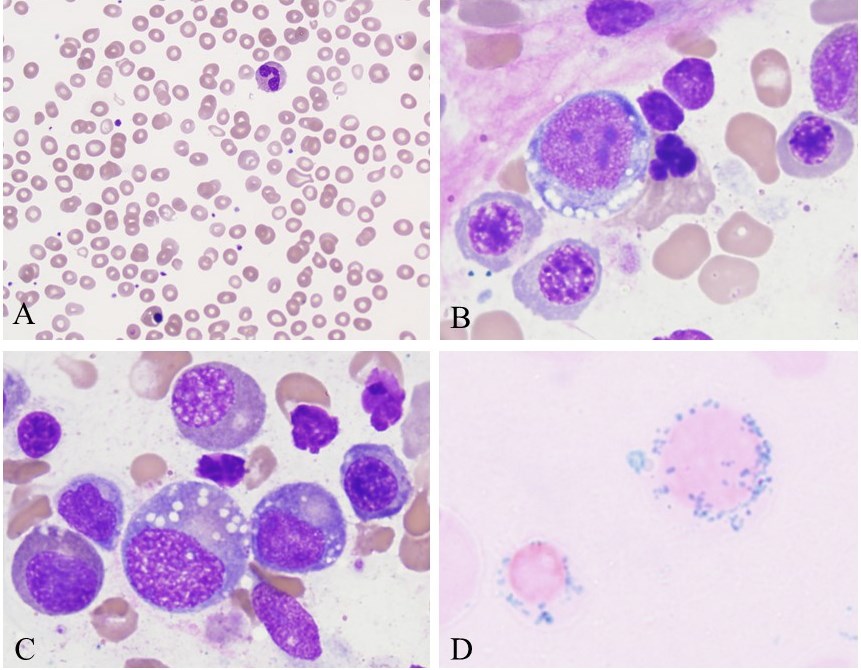
Case Presentation: A 54-year-old male with a history of Roux-en-Y gastric bypass surgery 12 years prior presented to the ED after labs showed a new pancytopenia from eight months prior. He reported fatigue but denied fevers, weight loss, dyspnea, bleeding, or recent infections. Medical history was notable for myocarditis 20 years ago and cholecystectomy 1 year prior and no significant family history. The patient was well-appearing with no vital sign or physical exam abnormalities. Labs were notable for Hb 7 g/dl (MCV 103), WBC count 1,700/microliter (ANC 170/microliterl), plt count 116,000/microliter, normal SPEP with hypogammaglobulinemia, normal LDH, ferritin, B12, zinc, and TSH. Peripheral blood smear demonstrated occasional pseudo Pelger-Huet WBCs, and few tear drop RBCs (Fig. 1A). Abdominal CT showed no lymphadenopathy, masses or hepatosplenomegaly. A bone marrow biopsy revealed a normocellular marrow with dyserythropoeisis, ring sideroblasts, left-shifted granulocytic maturation, cytoplasmic vacuolization in both erythroid and granulocytic precursors, and no increase in blast counts (Fig. 1B-D); cytogenetics and flow cytometry were negative for markers of myelodysplasia. After discharge, serum copper levels returned at <5 mcg/dl. The patient had been taking a multivitamin with 2mg of copper oxide, but serum copper levels and pancytopenia only improved after initiation of PO copper gluconate at an initial dose of 4mg TID by hematology. His copper dose has been slowly decreased since with no recurrence of cytopenias.
Discussion: Copper absorption primarily occurs in the stomach and proximal small intestine. While still exceedingly uncommon, Roux-en-Y gastric bypass surgery is a well-known cause of copper deficiency. Other conditions that can lead to copper deficiency include celiac disease, excessive zinc ingestion, and dependence on total parenteral nutrition. Copper is a co-factor for enzymes vital to hematopoiesis. Anemia and neutropenia can be seen in prolonged copper deficiency with or without neurologic sequelae. Bone marrow findings can mimic myelodysplastic syndrome (MDS) with findings of dysplasia, left-shift in granulocyte and erythrocyte maturation and ring sideroblasts. Cytoplasmic vacuolization occurs in both erythryoid and myeloid cells in copper deficiency, whereas it only occurs in erythroid precursors in MDS. Oral copper given at a high enough dose can reverse hematologic abnormalities. Notably, copper oxide has decreased bioavailabilty compared to other copper salt formulations.
Conclusions: Though copper deficiency following gastric bypass surgery remains uncommon, its occurrence can have significant hematologic effects and can mimic myelodysplastic syndrome. Cytopenias often resolve following supplementation, preferably with non-oxide copper salt formulations.