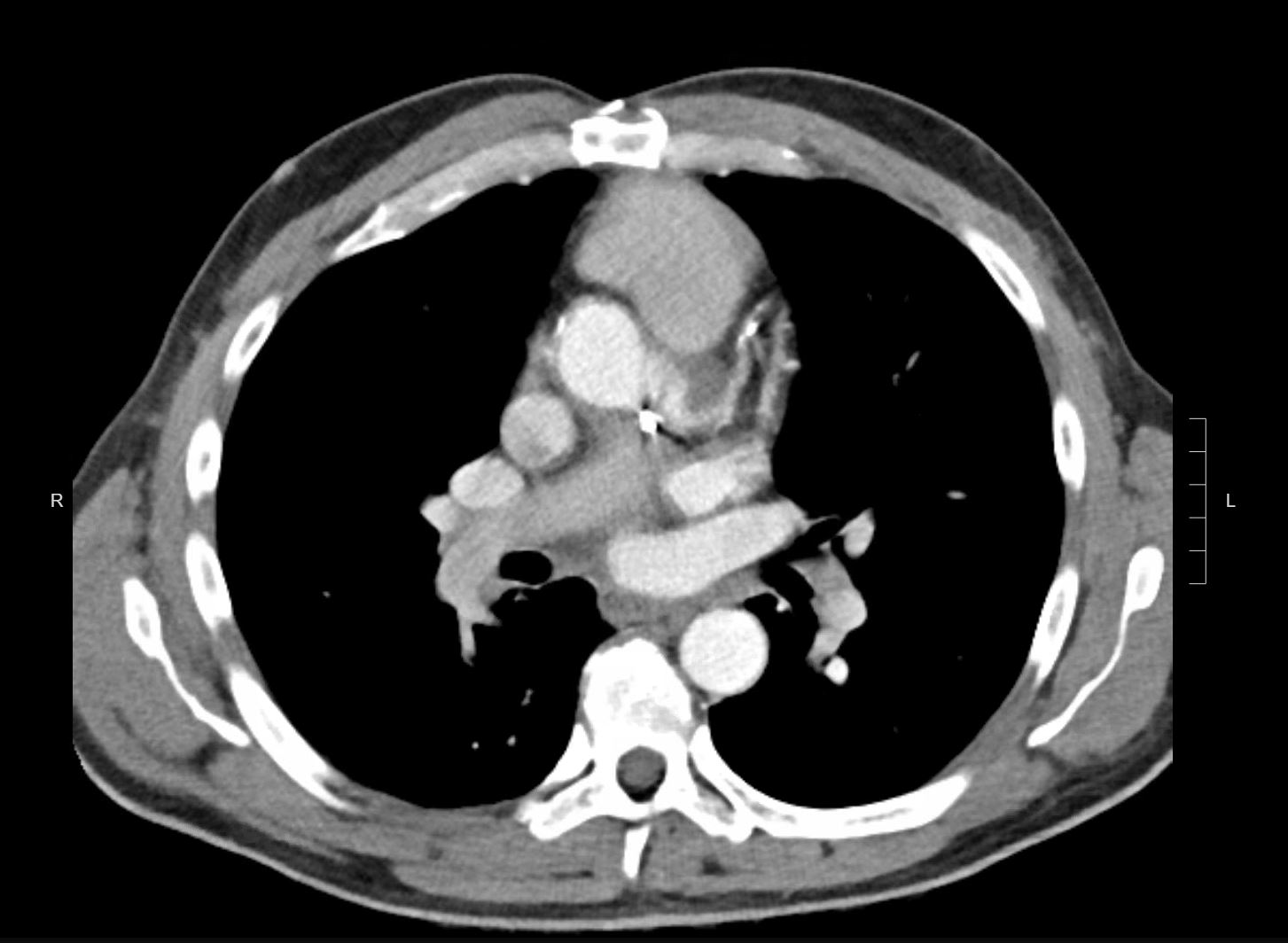
Case Presentation: A 55-year-old male with a remote history of intravenous drug use leading to aortic valve endocarditis and bioprosthetic aortic valve replacement, Bentall ascending aortic arch repair, and Micra leadless pacemaker placement, presented to his primary care physician with a petechial rash on his lower extremities. He noted several weeks of malaise and low-grade fevers. He was hospitalized for further evaluation. On admission, he had a low-grade fever of 99.5F with otherwise stable vital signs. Exam revealed a fatigued but well-appearing male in no acute distress. Cardiac exam was notable for a holodiastolic murmur at the right sternal border and a holosystolic murmur at the left lower sternal border radiating to the axilla. Skin exam showed multiple, erythematous, flat, nontender macules on the bilateral lower extremities and feet (see Image 1).Basic lab work showed a normal white blood cell count of 5.7 x 10^9/L, an elevated sedimentation rate of 59 mm/hr, and an elevated c-reactive protein of 10.1 mg/dL. Two sets of blood cultures grew Lactobacillus species. Rheumatologic labs including ANA, ANCA, anti-dsDNA, and rheumatoid factor were negative. Hepatitis B and C serologies were negative for infection. A transesophageal echocardiogram showed a peri-aortic abscess (see Image 2). Biopsy of the rash showed small vessels with thrombosis associated with acute inflammation composed by neutrophils, lymphocytes, and eosinophils, consistent with leukocytoclastic vasculitis.On further questioning, the patient had had dental work approximately one month prior to admission and had not taken prophylactic antibiotics nor had he been taking his chronic, suppressive Bactrim.The presentation was consistent with a diagnosis of Lactobacillus bacteremia and endocarditis causing a leukocytoclastic vasculitis. In consultation with infectious disease and cardiothoracic surgery, the patient was treated with intravenous penicillin G and underwent redo aortic valve replacement surgery. The rash resolved and the bacteremia cleared.
Discussion: Lactobacilli are rod-shaped, gram-positive bacteria found in the normal flora of the oropharynx and gastrointestinal and genitourinary tracts. Lactobacilli are rare causative agents of endocarditis. A literature review of 50 reported cases showed that predisposing factors include: valvulopathy (64% of cases), prosthetic valves (14% of cases), dental procedures (34% of cases), probiotic use (22% of cases), and immunosuppression (16% of cases). Morbidity and mortality of Lactobacillus endocarditis is high with 54% of patients requiring valve surgery and a 10% mortality rate. Most Lactobacilli are highly sensitive to penicillin. Antibiotic therapy for Lactobacillus endocarditis typically involves several weeks of IV penicillin G or an aminopenicillin. Clindamycin is an alternative agent for patients with a penicillin allergy.
Conclusions: This case demonstrates the importance of recognizing that a new-onset, vasculitic-appearing rash may require inpatient evaluation for bacteremia and endocarditis in the appropriate clinical context. It also reveals that Lactobacilli are a rare but serious cause of bacteremia and endocarditis in patients with recent dental work, valvulopathy, prosthetic heart valves, probiotic use, and/or an immunocompromised state.