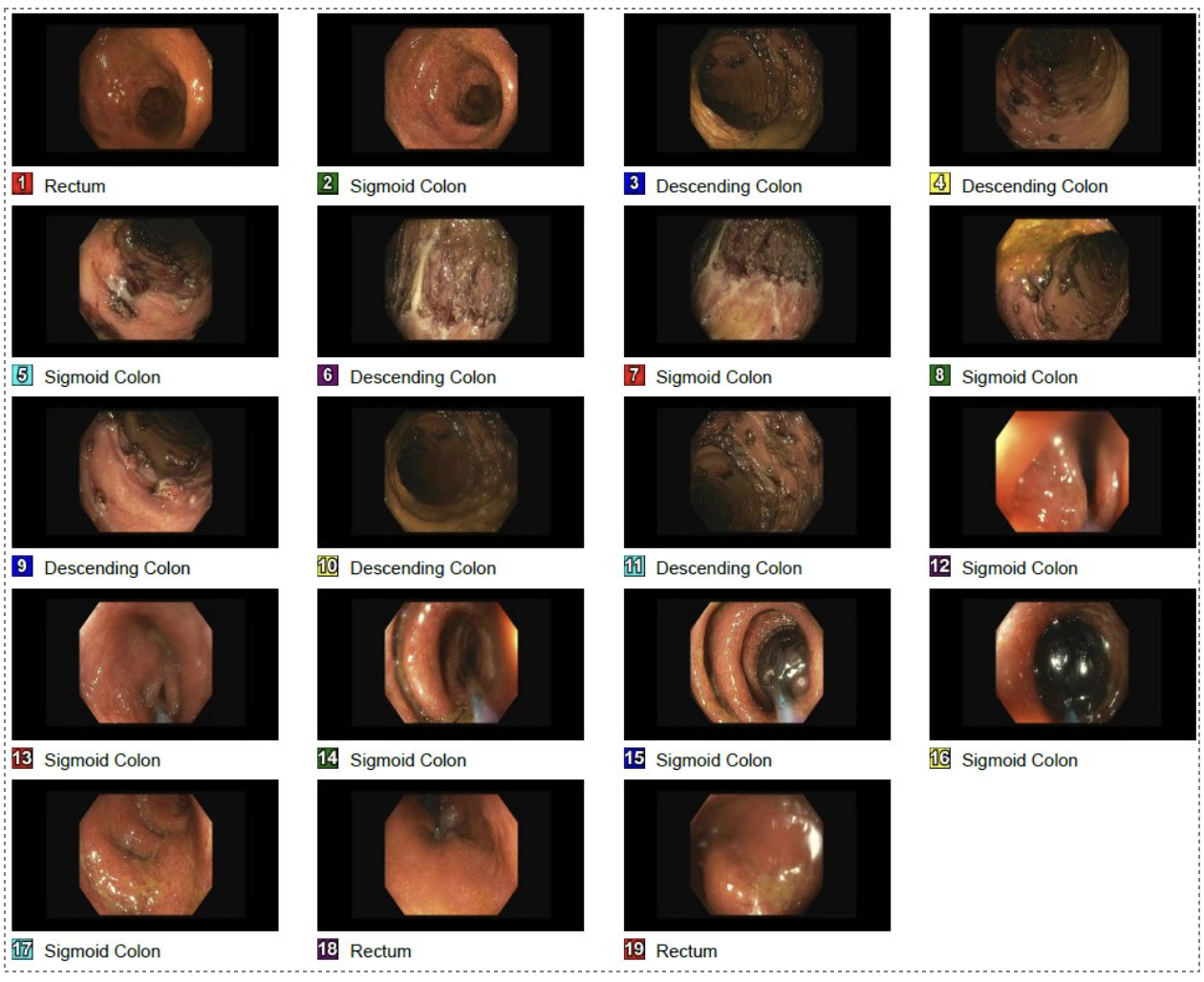
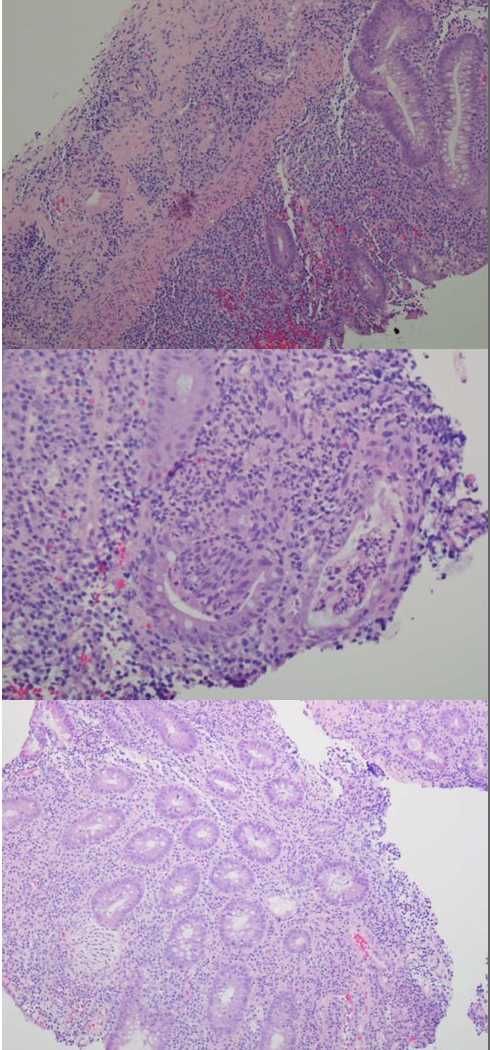
Case Presentation: 75 year old male with history of atrial fibrillation, COPD, CAD s/p CABG in 2018, diabetes and recent admission for diverticulitis presented with abdominal bloating, melena, decreased appetite and weight loss. On admission, his hemoglobin was 13 g/dl, white blood cell count 15/mm3 and CRP 136 mg/L. Initial CT A/P without contrast revealed diffuse wall thickening of the colon concerning for active colitis. The patient was started on ciprofloxacin and metronidazole but had unresolving symptoms and worsening leukocytosis necessitating broadened antibiotic coverage. Repeat CT A/P with contrast was performed which revealed a possible stricture versus neoplasm in the sigmoid colon. Flexible sigmoidoscopy then showed a benign-appearing, intrinsic moderate stenosis measuring 3 cm (in length) at the sigmoid colon which was dilated to 18 mm. Also noted at the time of sigmoidoscopy was inflammation and scarring with loss of vascularity in a continuous and circumferential pattern without any sites spared. Biopsies were positive for active chronic colitis of the descending colon and rectum. Due to involvement of the rectum and pathological findings suggestive of chronic inflammation, Segmental Colitis Associated Diverticulitis, SCAD, was eliminated from the list of differentials and severe ulcerative colitis (UC) was diagnosed. A few weeks later, he was re-admitted with sepsis and peritonitis. He developed a feared complication of UC, toxic megacolon, leading to colon perforation requiring total colectomy and end ileostomy. The patient declined post op and unfortunately passed away.
Discussion: Inflammatory bowel disease is at the forefront of differentials in younger patients presenting with abdominal pain and bloody stool. Ulcerative colitis (UC) has a bimodal age distribution with the second peak occurring between the ages of 50-70. Late onset is typically associated with more fatal complications, such as toxic megacolon. Similar in presentation to late onset UC is SCAD, a rare and often missed diagnosis that most commonly affects the sigmoid colon. A key differentiating feature of SCAD in comparison to UC is sparing of rectal mucosa. Both diagnoses are characterized by severe inflammation thus steroids play a vital role in management. Early identification of both disease processes can lead to appropriate initiation of steroid therapy which can alter clinical outcomes.
Conclusions: Though more commonly diagnosed in younger individuals, new onset ulcerative colitis can present in older adults and should be considered in patients that present with abdominal pain, bloody stool and weight loss. SCAD presents similarly and is often misdiagnosed as UC. It can be seen in patients with recent history of diverticulitis and is characterized by inflammation limited to the sigmoid colon without involvement of the rectum.