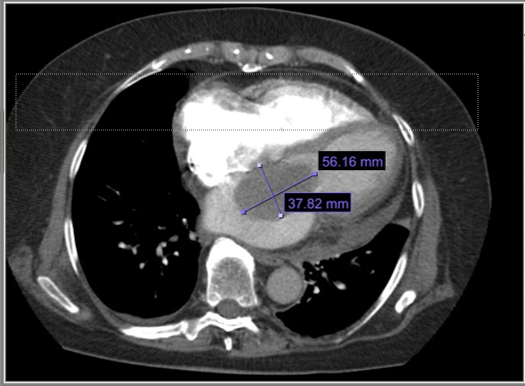
Case Presentation: This is a case of cardiac myxoma in a 78-year-old female with a history of atrial fibrillation on chronic anticoagulation. The patient presented to the Emergency Department with left-sided intermittent chest pain and a one-month history of exertional fatigue and dyspnea. Physical examination revealed a diastolic rumble in the left lower sternal border. Given the clinical presentation and elevated D-dimer, pulmonary embolism was initially suspected and ruled out with a computed tomography angiography (CT angio).The CT angio, while excluding pulmonary embolism, unexpectedly revealed a 5.7×3.8 cm soft tissue mass in the left atrium. Subsequent echocardiography confirmed the diagnosis of a large left atrial myxoma measuring 7.5 cm x 4.4 cm, which partially obstructed left ventricular inflow and caused functional mitral valve stenosis.The patient underwent cardiac catheterization, revealing normal coronary arteries, and was referred for surgical removal of the left atrial myxoma. Following successful resection, the patient experienced symptomatic improvement and was discharged on a medication regimen consisting of Metoprolol, Lasix, and Eliquis. She was advised to attend regular follow-up appointments to monitor her cardiac health and assess for any recurrence of the myxoma.
Discussion: A myxoma is a rare benign tumor of the heart. Depending on location and morphology, cardiac tumors can produce four types of clinical manifestations: systemic-constitutional, embolic, cardiac, and secondary metastatic manifestation. Two morphological forms exist: polypoid and papillary. Polypoid myxomas often present with obstructive features, while the papillary forms are more prone to embolization. In this case, the patient’s cardiac myxoma presented with symptoms such as exertional fatigue, dyspnea, and chest pain, which are consistent with the obstructive and embolic effects of the tumor. The presence of a diastolic rumble on physical examination was a notable clinical finding, but the initial suspicion of pulmonary embolism highlighted the challenges of diagnosing cardiac myxoma due to its diverse clinical presentations. Echocardiography is the investigation of choice. Echogenic polypoid or papillary mobile mass within the atrial cavity remaining attached to the interatrial septum through a stalk are the tell-tale echocardiographic features. Surgical excision of cardiac myxoma carries a low-operative risk and gives excellent short- and long-term results.
Conclusions: This case underscores the importance of considering cardiac myxoma in the differential diagnosis of patients presenting with cardiac symptoms, particularly when other etiologies, such as pulmonary embolism, are ruled out.Clinical manifestations of myxomas consist in a triad: constitutional symptoms, embolization and intracardiac obstruction. Early diagnosis and prompt surgical management are essential for improving patient outcomes and relieving symptoms associated with this rare cardiac tumor. As with this case here, the successful removal of the myxoma led to symptomatic improvement and underlines the curative potential of surgical intervention.