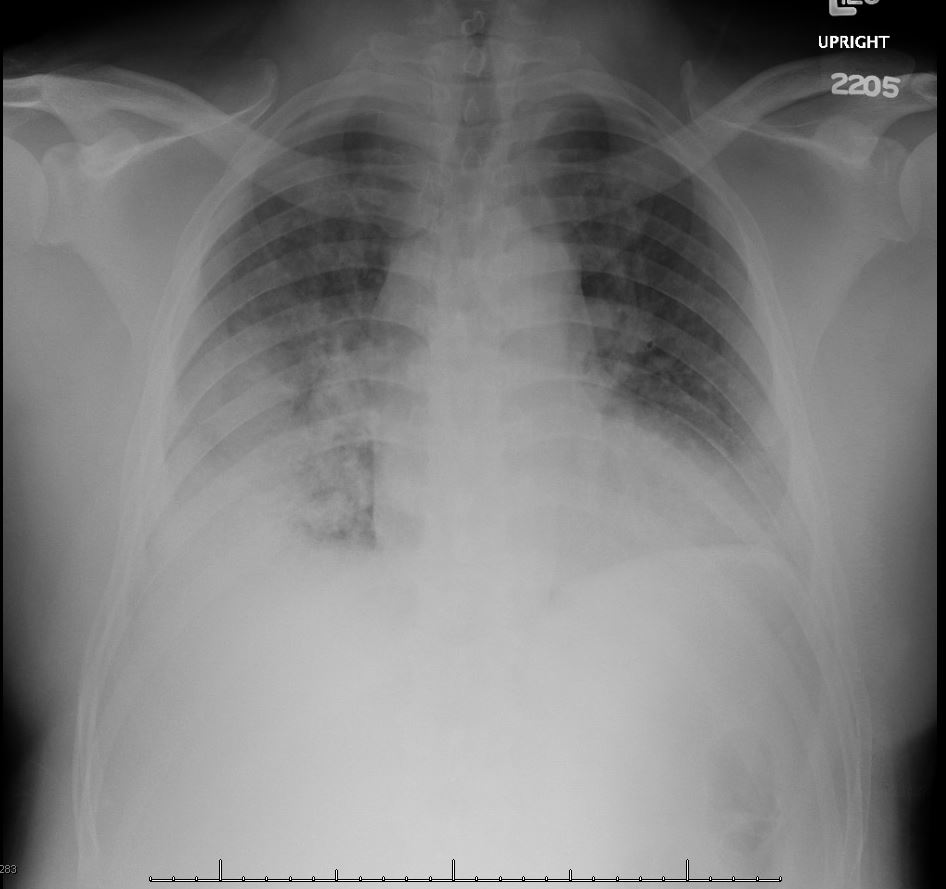
Case Presentation: A 43-year-old male with history of hypertension and alcohol abuse presented with a 3-day history of URI like symptoms including high grade fevers, cough productive of yellowish sputum, generalized abdominal pain, nausea and diarrhea. On physical examination, Blood pressure 136/83 mmHg, pulse 151 beats per minute, respiratory rate 24 breaths per minute, temperature 40.3 degrees Celsius, and O2 95% on room air. He had wheezes in both lungs, and exhibited abdominal distention and guarding. His white cell count 18.8 (4.5–11 × 103/uL); hemoglobin 13.3 (12–16 g/dL); platelet 272 (140–440 thou/cu mm); sodium 131 (135–145 mmol/L); BUN 13 (6–22 mg/dL); creatinine 1.78 (0.6–1.17 mg/dL); and creatine kinase (CPK) peaked at 5200 U/L (22–195 U/L). Urine analysis assay for Legionella antigen serogroup 1 was positive; blood culture and urine culture were without bacterial growth; respiratory viral panel was negative. Stool assay was negative for shigella, E Coli, campylobacter and salmonella. Electrocardiogram showed sinus tachycardia. Chest x-ray showed airspace disease within the anterior segment of the right lower lobe consistent with pneumonia. He was diagnosed with Legionella pneumonia, rhabdomyolysis, and acute renal failure. He was started on triple antibiotics therapy with azithromycin, ceftriaxone and metronidazole. Triple antibiotics therapy was initiated because of concern for superimposed aspiration pneumonia due to location of consolidation on chest x-ray. He was persistently febrile for 3 days in the hospital, thus, the decision not to de-escalate antibiotics therapy. Repeat chest x-ray on day 2 showed increased right lower lobe airspace disease with new left bibasilar airspace disease. His acute renal failure slowly responded to intravenous hydration and so did his urinary output. On discharge, after 4 days in the hospital, creatinine was 0.92 md/dL and CPK 4200 U/L. He was discharged home on 6 days of azithromycin to complete therapy. At 6 days follow-up in the outpatient setting, CPK was down to 184, with resolution of consolidation on chest X-ray.
Discussion: Pneumonia is the most commonly described manifestation of Legionella infection and is termed Legionnaires’ disease. Legionella can also cause a self-limiting acute febrile illness, termed Pontiac fever. Rarely, Legionella causes extra pulmonary infections such as cellulitis, abscesses, endocarditis, or meningitis. It is also recognized but a rare cause of rhabdomyolysis. Urine antigen test is a rapid, practical, and inexpensive method for the diagnosis of the disease, characterized by sensitivities of 70–90% and specificities approaching 100%. The exact mechanism of muscle injury caused by Legionella is still unclear, however, release of an endotoxin or exotoxin that causes rhabdomyolysis and direct bacterial invasion seem to be the most probable mechanisms.
Conclusions: Legionella pneumophila has been shown to be a recognized but a very rare cause of rhabdomyolysis with renal failure. Review of the relevant literature on reported cases show that early diagnosis and administration of appropriate antimicrobial therapy is associated with improved outcomes.