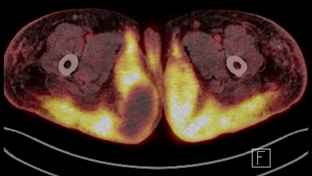
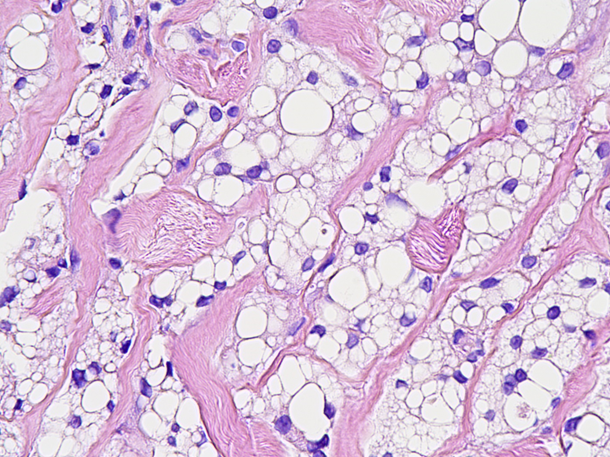
Case Presentation: A 76-year-old woman complaining with generalized edema underwent CT at a local hospital. It revealed diffuse subcutaneous edema and infiltration in pelvic area and both lower extremities and enlarged inguinal lymph nodes. She admitted our hospital for further evaluation. On physical examination, her vital sign was stable except high blood pressure of 172/88 mmHg. Not only Bilateral inguinal lymph nodes but also diffuse, firm subcutaneous mass-like lesions on her lower buttocks were palpated without tenderness. Laboratory results showed hypercalcemia (total calcium of 12.5 mg/dL and ionized calcium of 1.62 mmol/L) and azotemia (serum creatinine of 2.52 mg/dL). Serum parathyroid hormone level was low (lower than 5 pg/mL), while calcitriol and PTH-related hormone level were within normal range. FDG-PET scan taken to find a suitable site for tissue biopsy revealed diffuse hypermetabolic subcutaneous infiltration extending from pelvic area to both lower extremities (Fig 1). Through additional questioning, it turned out that the patient had silicone injection on both hip by a nonphysical individual 15 years ago. Gun biopsy was done from her left gluteal fold, and the histopathology showed numerous lipid vacuoles and fat necrosis, which is consistent with lipogranuloma (Fig 2). With suspicion of sarcoidosis, serum ACE level was measured, and it turned out to be high (>150 U/L). However, her histopathology showed only lipid-laden histiocytes, not palisading or epithelioid histiocytes which were usually seen in sarcoidosis. On working diagnosis of silicone granuloma, 20mg of methylprednisolone per day was given to the patient. Hypercalcemia and azotemia improved immediately, and after a few days the firm masses on buttock began to soften. After discharge, the patient reduced the dose of methylprednisolone to 2mg daily at outpatient clinic.
Discussion: Since first introduced in early 1960s, silicone implants and liquid silicone injections have been used extensively in cosmetic and reconstructive medicine [1]. Though silicone is chemically inert material, silicone implant leakage and free silicone injection can cause a variety of complications, ranging from local granuloma formation to silicone pneumonitis or diffuse systemic embolism [2]. Therefore, currently liquid silicone injection for soft tissue augmentation is in off-label use in USA [3]. While silicone granuloma is relatively common complication of liquid silicone injection or silicone implant, hypercalcemia is rarely accompanied [2]. To date, 15 cases of silicone induced hypercalcemia have been reported, and liquid silicone injections were used in all but one case [4]. As complete removal of injected silicone is usually impossible, medical treatment including bisphosphonate and steroid are used in most cases [4].In this case, lymphoma was initially considered as differential diagnosis because the patient had enlarged inguinal lymph node. After that, sarcoidosis was suspected due to hypercalcemia and elevated serum ACE level. However, her medical history and pathology made clear diagnosis for silicone granuloma, which showed thorough history taking and pathologic confirmation are important for accurately diagnosis and treatment.
Conclusions: Lipogranuloma caused by silicone injection can present with enlarged lymph nodes and hypercalcemia, mimicking sarcoidosis and lymphoma. Biopsy is essential for differential diagnosis.