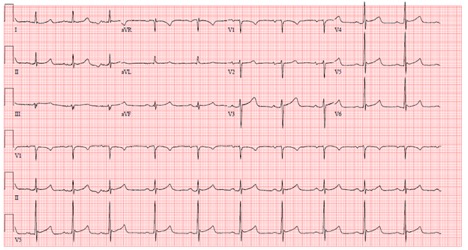
Case Presentation: A 61-year-old African American male with past medical history of type I diabetes mellitus, hypertension, benign prostatic hyperplasia, stage IV chronic kidney disease, and peripheral vascular disease presented to the hospital for altered mental status, lethargy, and hypoglycemia. Home medications included amlodipine, atorvastatin, ergocalciferol, insulin detemir, insulin lispro, lisinopril, sertraline and tamsulosin. After taking morning insulin and having breakfast, patient’s glucose was 56 mg/dL. Home attempts to increase blood glucose were unsuccessful. He felt increasingly ill and called EMS. On arrival to the ED, his oral temperature was 86F and other vitals were stable. Pertinent physical exam findings included ill appearance, clammy skin, and lethargy. Pertinent initial laboratory findings included WBC of 11.9×10^3/uL, hemoglobin of 11.2 g/dL, creatinine of 2.8 mg/dL (baseline 2.3), glucose of 92 mg/dL, and lactic acid of 2.5 mmol/L. A urinalysis and blood cultures were negative. A venous blood gas showed pH of 7.27, pCO2 of 54 mmHg, pO2 of 37 mmHg and HCO3 of 23.8 mmol/L. Chest x-ray showed low lung volumes with bronchovascular crowding and mild bibasilar atelectasis. An EKG demonstrated Osborn waves (Figure 1). External rewarming was initiated and patient was started on vancomycin, cefepime and metronidazole. Complete clinical resolution of symptoms was seen by day 2.
Discussion: Hypothermia, a body temperature below 95F (35C), has many different etiologies, including severe hypoglycemia, which is an episode that requires assistance to treat and has an incidence of 1-1.7 episodes per patient annually (6). Our patient had an initial blood glucose of 56 mg/dL. Hypothermia occurs as a compensatory mechanism to decrease energy demand and oxidative stress during glucose deprivation (7). The incidence of hypothermia in cases of severe hypoglycemia in patients with diabetes may be as high as 23%, irrespective of age or type of diabetes (5). Hypothermia is associated with significant morbidity and mortality (8,9). Therefore, implementation of rewarming methods should occur as soon as possible. The method utilized often depends on the stage of hypothermia. Passive external rewarming for mild (90F-95F; 32.2C-35C); active external rewarming for moderate (82.4F-90F; 28C-32.2C); and active internal rewarming for severe (<82.4F; <28C). Occasionally severe hypothermia requires extracorporeal rewarming (4). We utilized a Bair Hugger temperature management unitTM, a type of active external rewarming, for our patient which was successful in raising his body temperature.
Conclusions: Hypothermia may be a presenting sign of severe hypoglycemia in a patient with diabetes. It is a compensatory mechanism that may reflect the severity of hypoglycemia. Given the morbidity and mortality associated with hypothermia, rewarming techniques should be initiated as soon as possible. The type of technique used will often depend on the stage of hypothermia the patient is experiencing.