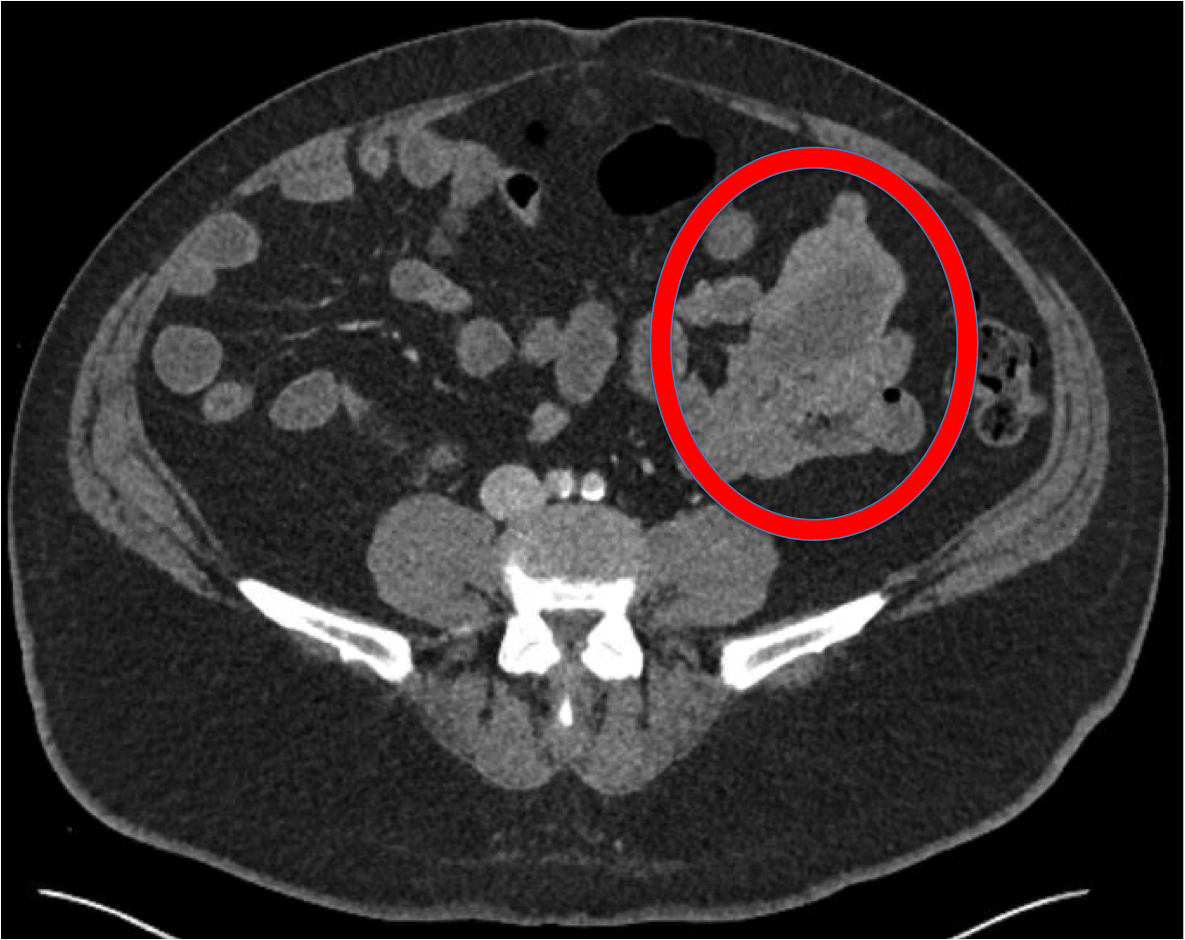
Case Presentation: A 56 year-old man with a history of psoriasis on adalimumab, coronary artery disease with prior stents, presented with chest pressure, dizziness, and dyspnea on exertion after noticing three days of melena and crampy abdominal pain. He denied nausea, vomiting, hematemesis, or bright red blood per rectum. Other than taking aspirin 81mg once daily, he took no other NSAIDs or anticoagulants.On exam he was afebrile, with a heart rate of 124, blood pressure of 144/65, breathing 22/minute, and saturating 99% on room air. He appeared pale. He was tachycardic without murmurs and his lungs were clear. Abdomen was soft with a reducible ventral hernia, with mild tenderness to palpation in the lower quadrants. Rectal exam revealed melena. His hemoglobin was 7.8 g/dL (down from baseline of 14 g/dL), BUN of 21 mg/dL, and creatinine of 0.9 mg/dL. He was given one unit of packed red blood cells and an urgent EGD revealed mildly nodular mucosa in the stomach, a normal duodenum, and no signs of active bleeding. Subsequent colonoscopy showed red blood in the terminal ileum and entire colon but no obvious source of bleed. Capsule endoscopy showed blood in the mid jejunum with no obvious lesions. He required three more units of blood during his stay until his melena resolved and his counts stabilized. Plans were made for an outpatient double balloon enteroscopy to evaluate his jejunum. Unfortunately two days later he had recurrent melena and his hemoglobin dropped to 6.2 g/dL. After another transfusion, he underwent a CT angiography that showed no active bleeding but did reveal a 6.4 x 4.6 x 5.4 cm mass associated with multiple loops of jejunum. Double balloon enteroscopy revealed a large submucosal mass with surrounding ectatic vessels seen with no stigmata of bleeding in the mid-jejunum. Given large vessels, biopsies were deferred. General surgery was consulted and he underwent an exploratory laparotomy where multiple small bowel masses were found, presumed to be hamartomas. Pathology revealed multifocal gastrointestinal stromal tumors (GIST) (see figure). The patient’s hemoglobin stabilized and he no longer required further transfusions. He was referred to oncology for consideration of systemic imatinib.
Discussion: GI stromal tumors (GIST) are rare with an incidence in the U.S. of ~4.3 per 1,000,000 per year. Gastric tumors make up 60-70% of cases. They are less commonly found the small intestine (20%-30%), the colon (5%), and the esophagus (<5%). Small intestinal GISTs are more likely to be malignant and aggressive. Patients may have symptoms related to bowel obstruction and occult bleeding. Acute hemorrhage is less common. Most GISTs are positive for CD117, which corresponds to the presence of the c-tyrosine kinase receptor (TyrK). GIST treatment involves surgical resection with intent for cure if localized, and systemic therapy with TyrK inhibitor (Imatinib) if metastasized. Prognosis is favorable for localized disease, but patients with metastatic disease have an average survival of only 19 months.
Conclusions: Hospitalists should acquire surgical consultation early to evaluate and treat GI bleeding associated with a mass, as both resolution of bleeding and a diagnosis can be achieved with one intervention. Though small bowel bleeding makes up only about 5% of all GI bleeding events, and of those the majority are related to AVMs, small bowel tumor related bleeding should always be considered. GISTs arising from the small bowel can be aggressive, and the mainstay of therapy includes surgery and a tyrosine kinase inhibitor.