Background: Dyad round means when nurses and doctors do patient round together. When the concept of hospitalist came to health care system, doctors became available 24 hours in the care of patients. Nurses and doctors started doing their patient-rounds individually1 and communicate via electronic medical record (EMR) or other electronic methods.On an average, a patient encounters 17.8 healthcare professionals during their hospitalization in medical floor2. Since patient contact with nurses are more than any other professionals of the care team2, nurses are the main source of information for patients and doctors. If doctors and nurses are not in unison while giving plan of care to patients, they become confused about their care which is reflected in patient experience score 1. Medical Error is the third leading cause of death in the USA3. Most cases of medical mistakes start with a miscommunication among members of care team3. Monash et al proved that integration of nurses in attending round improves patient experience4. Laufer and Prasad shared their quadruple aim of high quality, low cost, improved patient experience, doctors and staff satisfaction via Nurse-Physician rounding1.Our aim of Dyad round was improvement of “communication of doctors and nurses with patients” and domain of “time spent by doctors with patients” of Press Ganey post discharge survey believing this will improve overall patient experience.
Methods: We implemented Dyad round in patients of internal medicine hospitalist in community based non-academic 300-bed hospital from March 5, 2019. Data is taken from Press Ganey post discharge survey of HCAHPS (Hospital Consumer Assessment of Healthcare Providers and Systems) score from April 2019 to June 2019. We did Quasi-experimental design: Time Series studies with multiple results before and after intervention. There was no selection bias due to the inclusion criteria. Two main measurements are 1. Percentage of Dyad round actually happened: Round is counted asking nurses if they could do the round together, maintained check mark in a form by an in-charge nurse. 2. Measurement of Outcome: HCAHPS score.
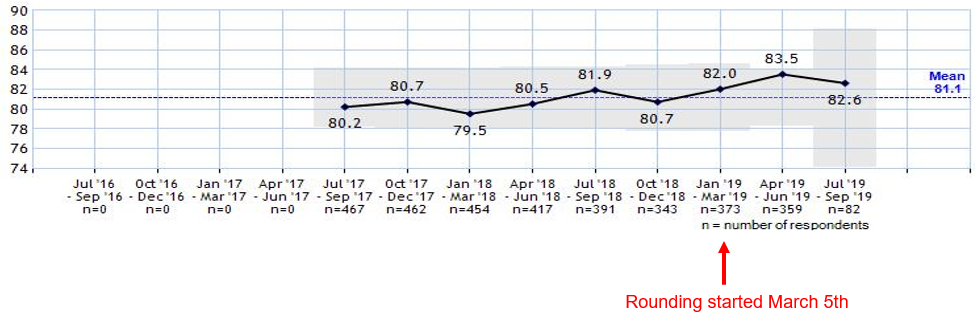
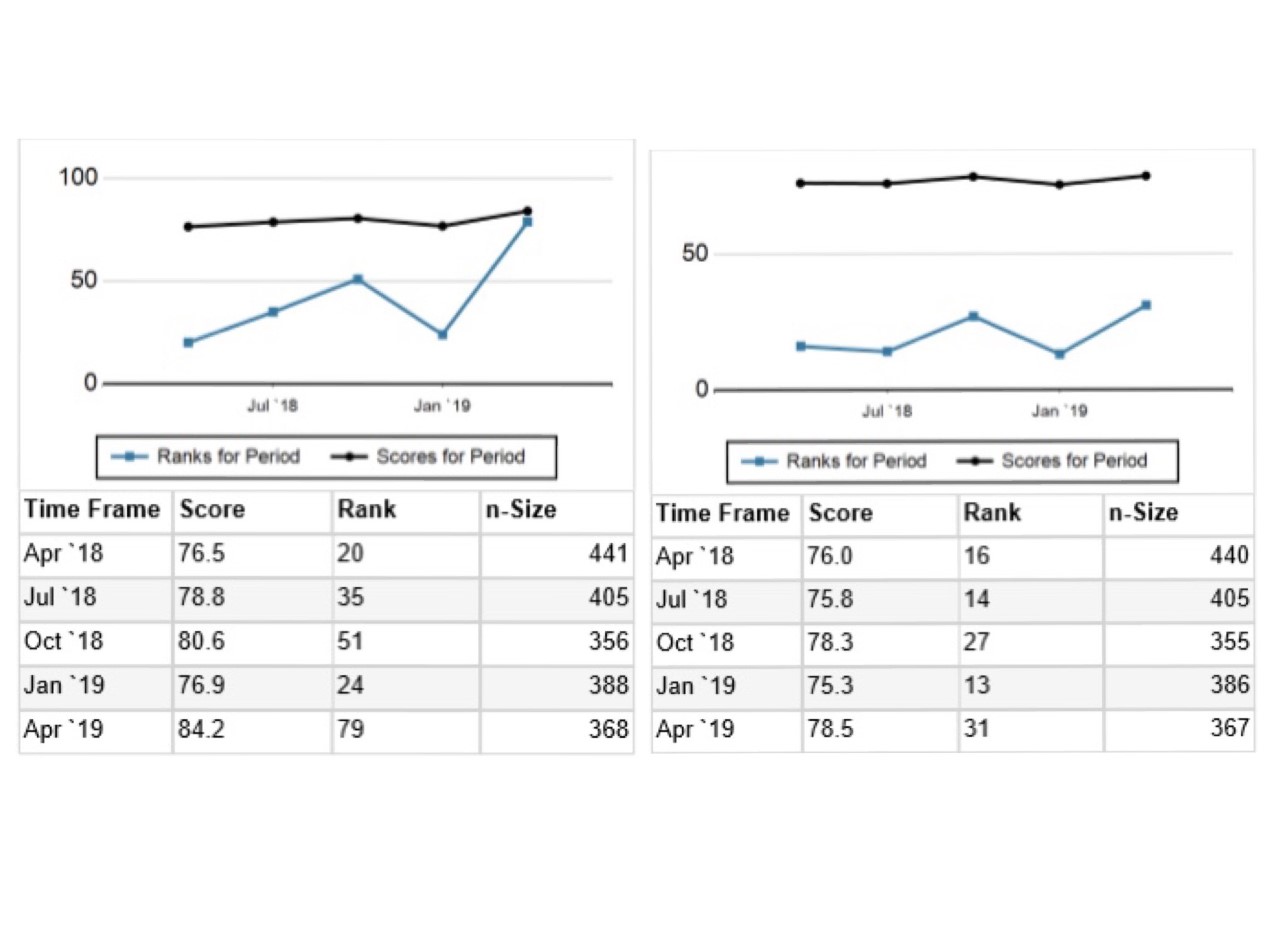
Results: In first 4 months of implementation 80.2% patients of internal medicine hospitalist were seen by Dyad round.HCAPS score showed improvements of time spent by doctors from 80% (n=373) to 83.5% (n=359) , communication with doctors from 75.3 (n=386) to 78.5 (n=367), communication with nurses from 76.9 (n=388) to 84.2 (n=368), and overall hospital performance from 86.5 (n=389) to 88 (n=368). Other positive improvements in HCAPS score are hospital rating from 69.9 (n=385) to 74 (n=366), communication about medicines from 57.9 (n=246) to 60.9 (n=233), response of hospital staff from 63.6 (n=353) to 70.1 (n=339), visitor and family from 87.1 (n=371) to 89 (n=351) and overall assessment from 90 (n= 384) to 91.2 (n=363). Some of the unmeasured results nurses and doctors shared are reduced pager for doctors, both hospitalists and nurses like working together. There is less misunderstandings, animosity, and better documentation in nursing charts.
Conclusions: Communication improves patient experience in the hospital 5. Our main aim of implementing Dyad round was to improve time spend by doctors with patients and communication of patients with doctors and nurses. Improvement of different domains of HCAPS score including out aim showed that Dyad round could be the magic wand for overall hospital performance and patient experience in hospital care.