Background: As a strategy to address its ongoing capacity crisis, our hospital has focused on reducing length of stay and improving throughput. Our hospitalists care for patients on >20 nursing units across four buildings, which creates inefficiencies that may prolong length of stay. Although other institutions have demonstrated improved patient flow by geographically cohorting patients and providers, prior efforts to implement geographic localization at our hospital have been unsuccessful.
Purpose: To thoughtfully design a feasible, effective, and sustainable geographic localization initiative among Hospital Medicine (HM) teams to improve efficiency, quality, and patient experience.
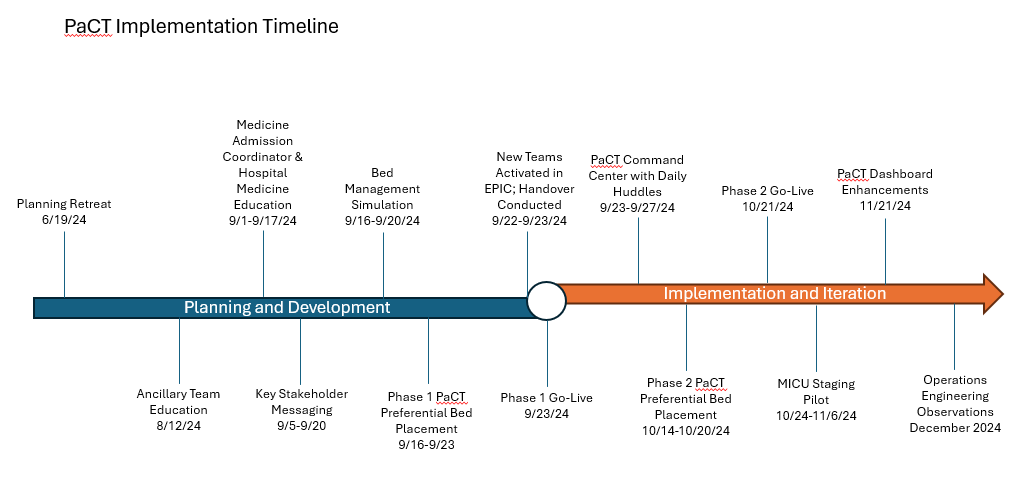
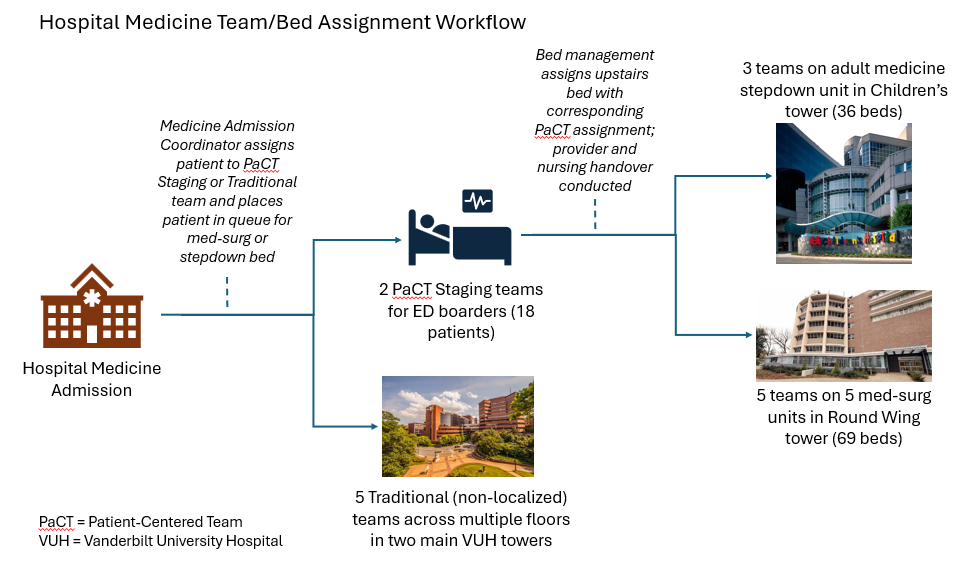
Description: The Patient-Centered Teams (PaCT) initiative was designed based on lessons learned from our previous localization efforts, insights from other institutions, and detailed local knowledge of hospitalist and bed management workflows. The hospital President and Chief Operating Officer served as executive sponsor and allocated project management, operations engineering, and analytics support. Stakeholders from physician leadership, nursing, clinical operations, bed management, transition management, and the Emergency Department were engaged. A half-day retreat was used to create future state process maps, and workgroups met weekly for three months to define standard operating procedures, educational materials, and key performance metrics. Messaging to frontline personnel about workflow changes occurred early and often during this period. Figure 1 details the implementation timeline. Phase 1 of PaCT implementation included localization of five HM teams paired with five nursing units in one tower. The target rounding census of attending-only teams post-implementation was 12 patients, which was a reduction from prior expectations. Phase 1 also included the creation of two HM staging teams, each responsible for rounding on, and advancing the care of, up to 9 Emergency Department boarders. PaCT phase 2 localized the assignments of three HM teams to a 36-bed medicine stepdown unit in a separate tower. Bed management processes were reengineered to assign appropriate patients to HM staging teams until a bed was available, at which time the corresponding PaCT team was designated, and provider and nursing handovers were conducted. Figure 2 depicts this workflow. After implementation, PaCT units/teams comprised approximately two-thirds of HM teams and patients. PaCT teams were accurately localized at a rate of >95%. Notable challenges included navigating the learning curve of bed management staff, ensuring fair distribution of work for non-localized HM teams, and managing assignments for patients transferring out of our closed medical intensive care unit. Compared to pre-implementation, PaCT teams saw a reduction in hospital length of stay, an increase in early discharges, and improved patient experience following localization. Qualitative feedback from hospitalists, nurses, and case managers was favorable.
Conclusions: A multidisciplinary team successfully designed and implemented a large systems change across Hospital Medicine to geographically cohort patients and providers to designated nursing units. Initial indicators of efficiency and patient and care team satisfaction have been positive. Optimization of provider and bed management workflows and assessment of impact on additional process and outcome measures are ongoing.