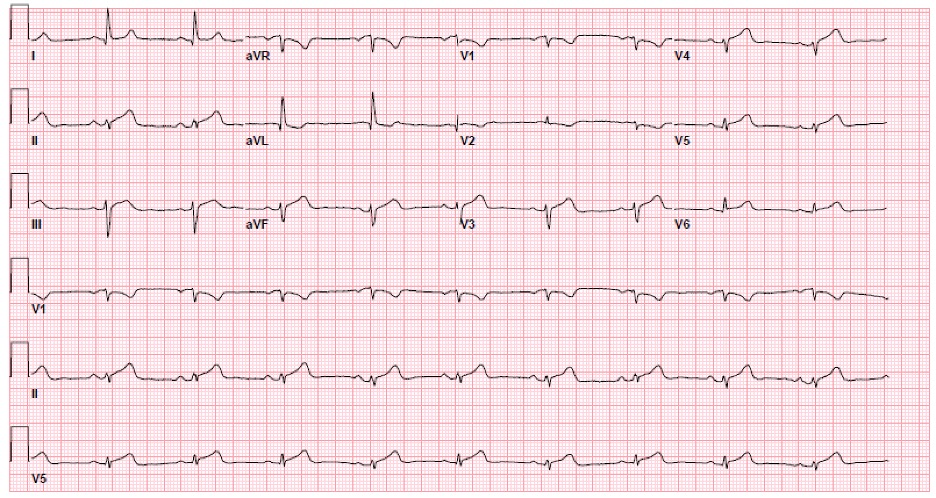
Case Presentation: A 63-year-old woman with a history of Lynch Syndrome who presented with acute chest pain. Her Lynch Syndrome manifested with invasive moderately differentiated adenocarinoma of the sigmoid colon managed with hemicolectomy as well as 9 cycles of Leuocoverin, 5-Fluorouriacil (5-FU) and oxaliplatin (FOLFOX) and prophylactic total hysterectomy and bilateral salpingo-oophorectomy. She completed her FOLFOX regimen just under 5 years prior to this acute chest pain episode. Having had no major events since remission, the patient presented to the emergency room after having acute substernal chest and left shoulder pain. Vitals signs were stable. Initial troponins were 3.194 then 23.093 ng/ml (normal < 0.03ng/ml). EKG demonstrated ST elevations in the inferior leads requiring urgent catheterization. She was found to have apical akinesis and non-obstructive coronary artery disease with a mild dissection of the left anterior descending artery, consistent with spontaneous coronary artery dissection (SCAD).
Discussion: SCAD accounts for 0.49% of all acute coronary cases and classically presents with acute chest pain and ST elevations in young females with no history of coronary artery disease. It is caused by an intimal tear in the coronary artery ultimately leading to dissection. Therefore diseased intima is often the culprit to this presentation. Our patient had minimal cardiac history however she did have a history of exposure to a cardiotoxic chemotherapy agent. 5-FU is the second most cardiotoxic chemotherapeutic drug. A review of 37 studies, including prospective studies to phase III control trials, found the rate of any cardiotoxic event between 0.3 to 34% of patients. 5-FU is a fluoropyrimidine that can cause cardiac free radical damage, direct endothelial injury and smooth muscle dysfunction. When this smooth muscle dysfunction affects the coronary arteries it can lead to vasospasm events, myocardial infarctions, and akinesis. One study of cardiotoxicity in 5-FU showed a 4-fold increase in all cardiac events. It has been shown that further risk factors for cardiotoxicity related to 5-FU administration include polychemotherapy (especially including a platinum based agent), and continuous infusion of 5-FU (as opposed to bolus infusion). Cardiotoxic events tend to occur during the first cycle of 5-FU. A previous case study demonstrates 5-FU as the culprit of SCAD in a young woman with active anal cancer when she presented with acute chest pain only 4 days after 5-FU. However our patient was well in remission, with treatment completed 5 years prior to her cardiac event. SCAD presents abruptly with no insidious events, therefore we propose that there is a link between potential smooth muscle dysfunction secondary to her 9 cycles of 5-FU predisposing her to intimal tears.
Conclusions: In summary, in a patient with a prior oncological history treated with 5-FU presenting with acute chest pain one must include SCAD in the differential.