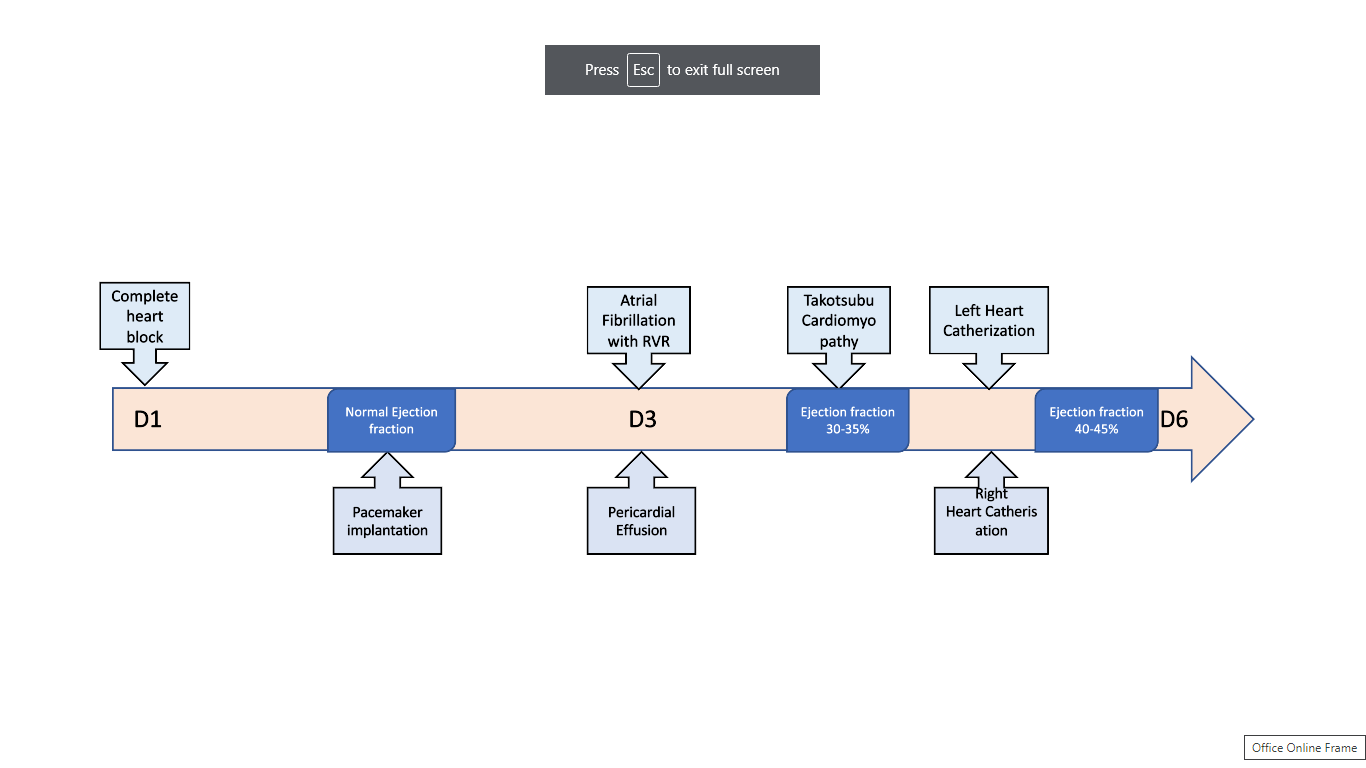
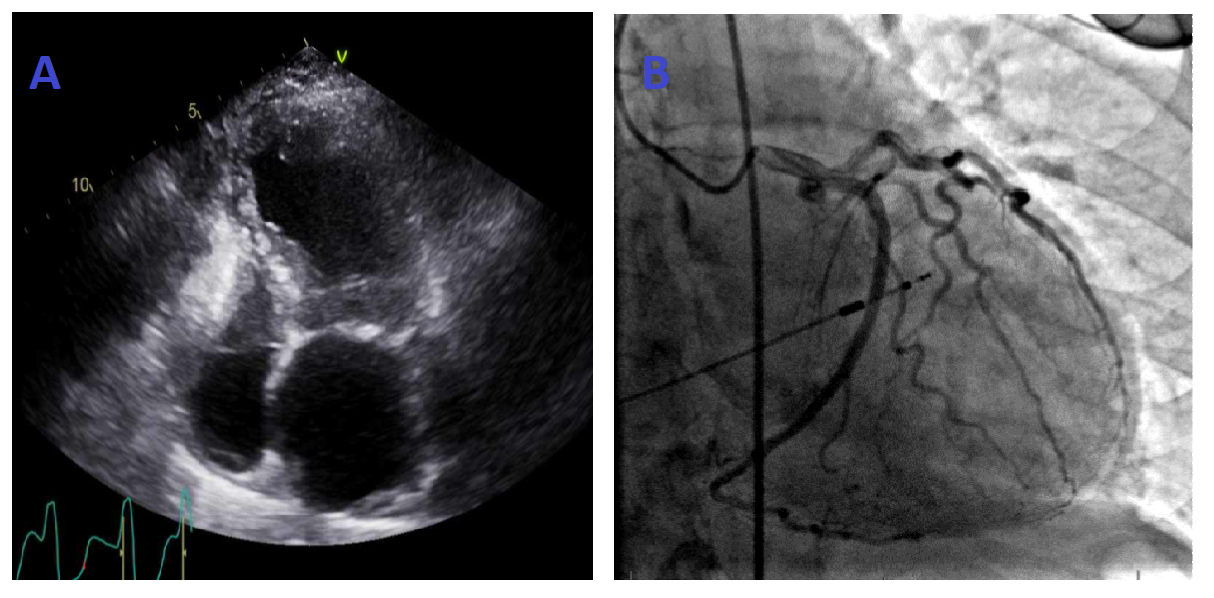
Case Presentation: Our patient is 78-year-old female with a history of mitral regurgitation, left ventricular outflow tract obstruction (LVOT) with systolic anterior motion (SAM) of mitral valve, migraines, and hypertension presented with lightheadedness. She had increased blood pressure at her recent office visit few weeks back necessitating an increase in dosage of verapamil. At presentation, patient was bradycardic with heart rate of 45/min and hypotensive with blood pressure of 75/32 mmHg. Electrocardiogram (EKG) was suggestive of complete heart block, left bundle branch block, and junctional escape rhythm. As she qualified the criteria, a dual-chamber pacemaker was inserted for intermittent complete heart block. About 12 hours after the procedure, patient was noticed to be in atrial fibrillation with rapid ventricular response with underlying left bundle branch block. Due to hypotension, she was started on amiodarone drip. Additional workup revealed elevated troponin peaking at 14 ng/ml. Transthoracic echocardiogram (TTE) was remarkable for reduced ejection fraction (EF) of 30-35% with wall motion abnormalities suggestive of Takotsubo cardiomyopathy along with small pericardial effusion and moderate to severe mitral and tricuspid regurgitation. Ejection fraction on TTE pre-procedure was >70%. Patient was initiated on heparin drip for non-ST segment elevation MI (NSTEMI) and stroke prophylaxis for atrial fibrillation. She underwent cardiac catheterization which showed non-obstructive coronary vessels ruling out coronary artery disease as etiology for decreased ejection fraction. Patient was started on and tolerated beta-blocker. She was discharged home on oral amiodarone, metoprolol, and apixaban.
Discussion: Cardiac Implantable Electronic Devices (CIED) like pacemakers have frequently been used for the treatment of bradyarrhythmias. Although these CIEDs are lifesaving, they are associated with a myriad of post-procedure complications. The case described above highlights one of the complications of permanent pacemaker implantation, Takotsubo cardiomyopathy. Hospitalists frequently admit patients undergoing implantation of these devices and should be aware of Stress/Takotsubo cardiomyopathy as a complication in post-operative period.
Conclusions: Cardiac Implantable Electronic Devices (CIED) are associated with short- and long-term complications which are associated with increased morbidity, healthcare costs, and mortality. Patient and procedure-related variables influence the outcome of post-procedure complications1. More research is required to establish risk stratification tools to evaluate the quality of CIED placement and to identify patients at high risk.