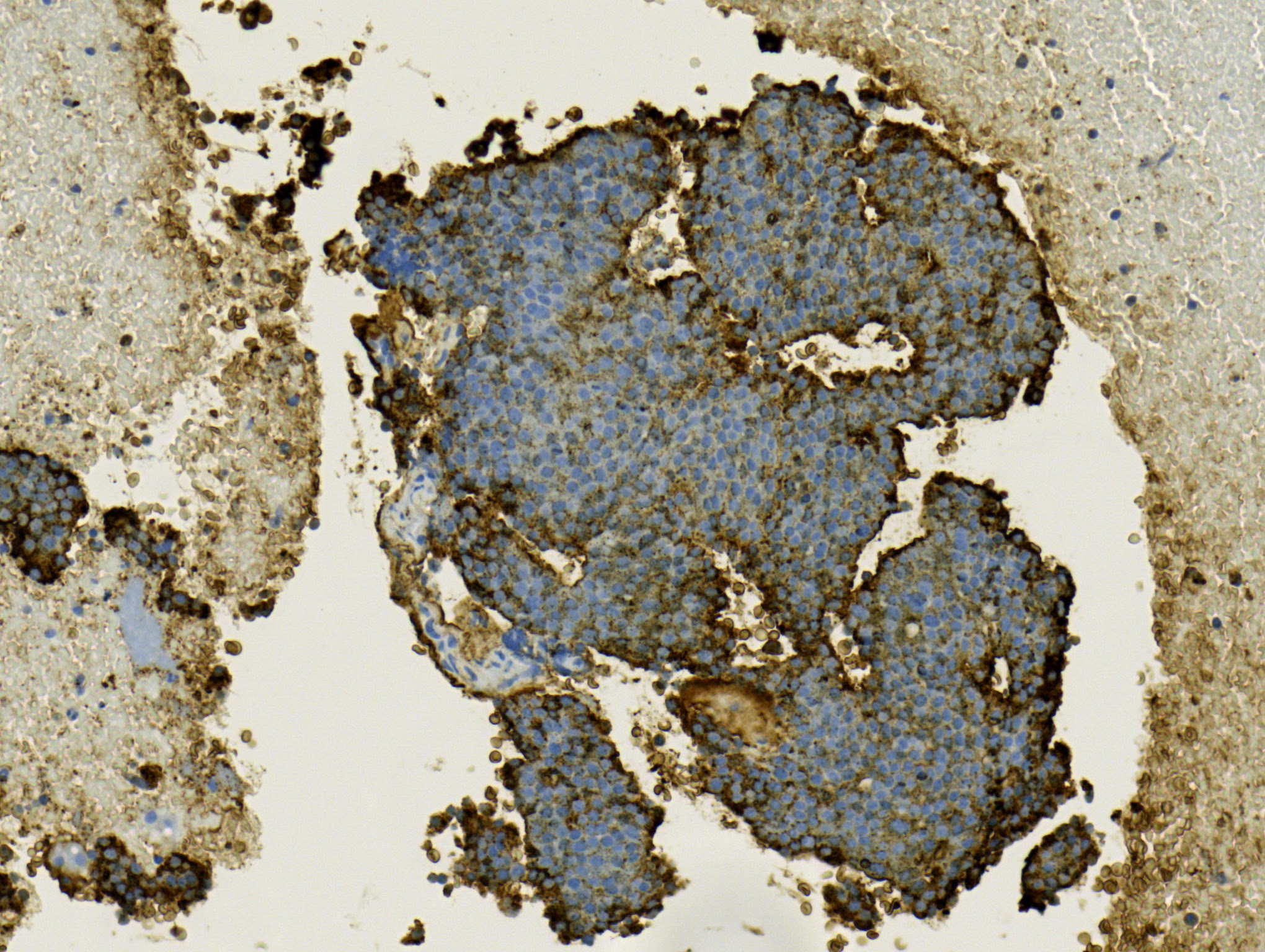
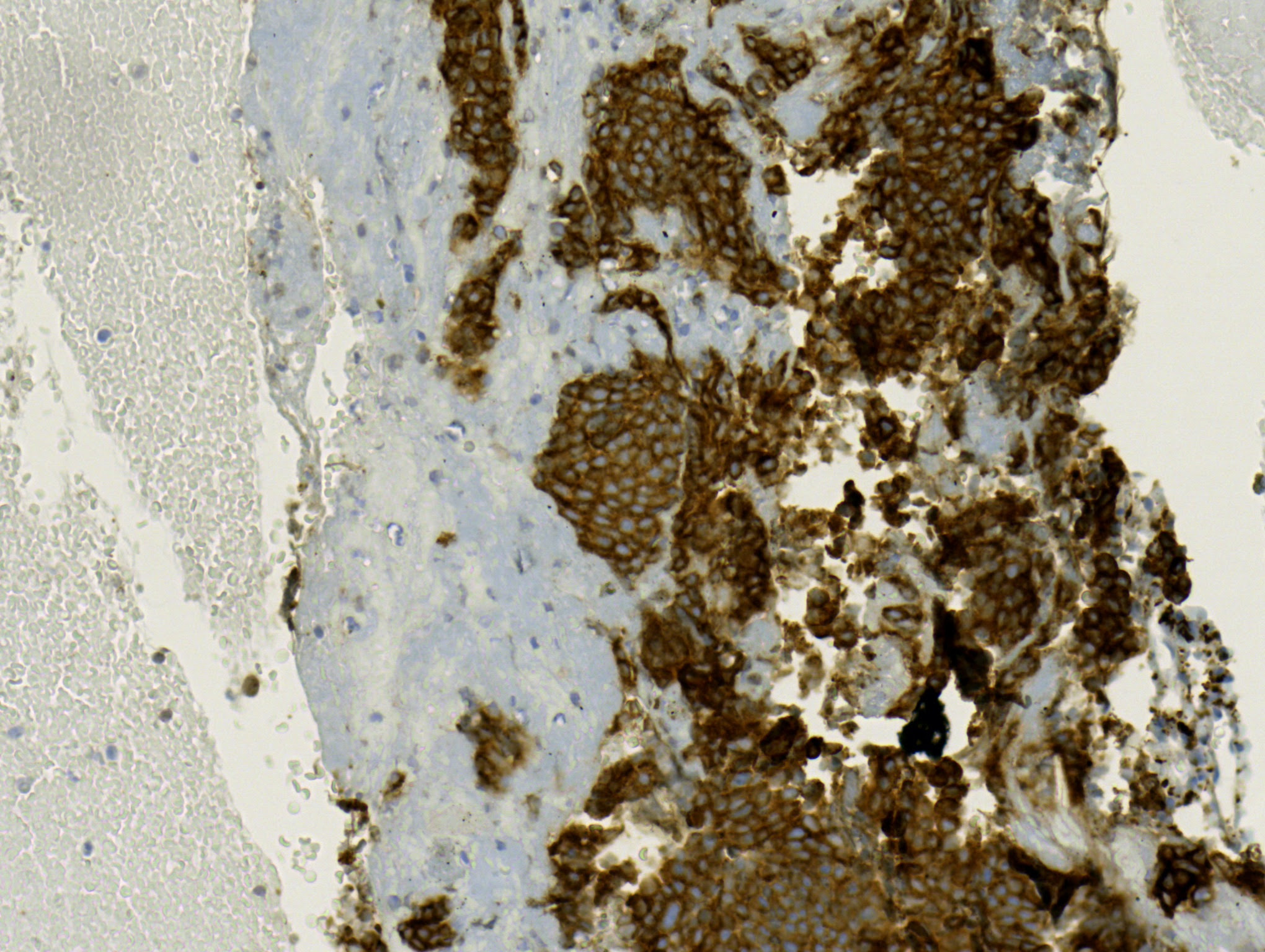
Case Presentation: We present a case of a 58 year old female with complaints of abdominal pain. The patient had six months of alternating fevers, chills and fatigue. She was placed on antibiotics but her fevers returned upon completion. Three months thereafter, the patient developed left lower quadrant abdominal pain that was sharp in nature and radiated to her groin. A CT scan of the abdomen and pelvis demonstrated an enhancing soft tissue mass with internal cystic and necrotic changes located in the midline upper pelvis, measuring 2.8 by 2 cm and two adjacent satellite nodules located superior to the mass. The location of this mass made it un-amenable to a percutaneous biopsy. The patient underwent an Endoscopic Ultrasound Guided Fine Needle Aspiration (EUS-FNA) with cytology demonstrating low grade neuroendocrine carcinoma with the malignant cells being positive for chromogranin A and synaptophysin. Endoscopic evaluation was negative. A capsule endoscopy revealed two small areas in the jejunum that were concerning for small bowel tumors. A subsequent octreoscan was positive, showing an abnormal activity in the mid-abdomen. The patient subsequently underwent surgical excision. The surgical pathology confirmed the mesenteric mass finding as metastatic low grade neuroendocrine tumor and identified two distinct small bowel low grade carcinoid tumors.
Discussion: Neuroendocrine tumors (NETs), also known as carcinoid tumors, are epithelial neoplasms that arise from enterochromaffin cells and are classified according to their histologic features and confirmed by immunohistochemical staining. NETs most commonly occur in the gastrointestinal tract, pancreas, appendix, rectum and the lungs but they can develop anywhere in the body. Due to their common embryonic origin, neuroendocrine tumors of the jejunum, ileum and appendix are collectively called midgut carcinoid tumors. NETs are now the most common small bowel tumor. Small bowel NETs are difficult to diagnose as they follow an insidious course; early on in the disease, symptoms are vague and nonspecific. Late diagnosis when regional or distant metastasis have already occurred is common. Forty percent of symptomatic patients without carcinoid syndrome present with vague abdominal pain.
Conclusions: Carcinoid tumors can vary in their presentation and delay the time of diagnosis. Early consideration for NETs in the differential for patients with vague undiagnosed abdominal symptoms could lead to more prompt diagnosis and treatment prior to metastatic spread.