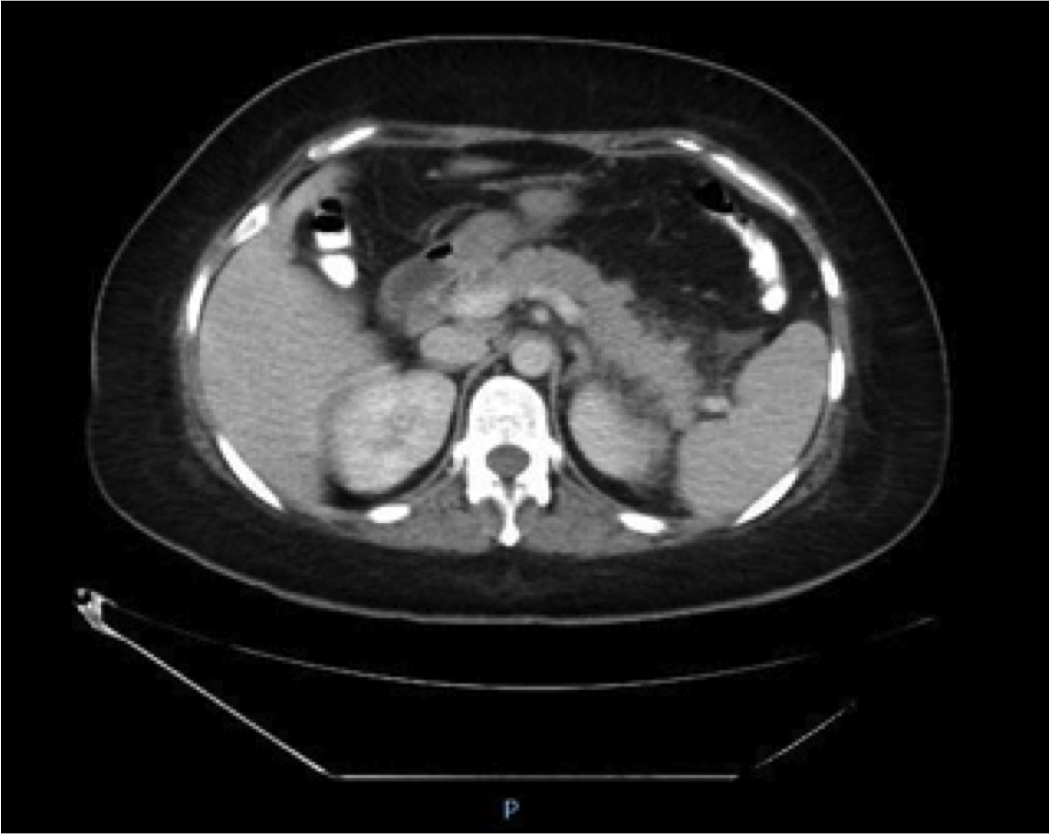
Case Presentation: A 41-year-old female presented with symptoms of abdominal pain, nausea, and vomiting one week after starting Methimazole 10 mg daily for Graves’ disease. She had no prior history of alcohol use or cholelithiasis. Her physical examination was significant for tenderness to superficial and deep palpation in her epigastrium. Her labs revealed a lipase level of 2457 (14-60) with normal liver function tests, normal triglyceride and calcium levels. Ultrasound of her abdomen showed no gallstones. CT scan of her abdomen confirmed a diagnosis of acute pancreatitis with evidence of pancreatic tail fat stranding. MMI was stopped on admission and other causes of acute pancreatitis were ruled out based on history, clinical presentation, labs, and imaging. She was treated with aggressive fluid resuscitation and kept NPO due to nausea. Intravenous opioid analgesics were administered to control her abdominal pain. Patient responded well to supportive therapy after discontinuation of MMI. She was re-challenged with MMI two days later with recurrence of symptoms including abdominal pain, nausea, and vomiting. A repeat elevated lipase level of 204(14-60) was noted. MMI was discontinued once more with complete resolution of her symptoms. In order to continue management of her Graves Disease, she was started on Propylthiouracil(PTU), Propranolol, and Dexamethasone. There is no known cross reactivity between PTU and MMI in causing acute pancreatitis. The patient eventually underwent a total thyroidectomy. She remained symptom-free through the rest of her hospitalization and was discharged home after being started on Levothyroxine.
Discussion: Acute pancreatitis is a serious medical condition responsible for up to 230,000 hospital admissions per year. However, drugs are responsible for only 0.1-0.2% of those causes. Methimazole has been known to cause other side effects but pancreatitis caused by methimazole is very rare. A definitive diagnosis involves the following 4 criteria: (a) development during the administration of the drug, (b) resolution after cessation of the offending drug, (c) recurrence after re-challenge of the suspected drug, and (d) exclusion of all other common causes. We achieved all four in this patient.
Conclusions: This case illustrates the importance for physicians to have a high index of suspicion for drug-induced pancreatitis caused by methimazole in the presence of classic symptoms. The clinician should discontinue the drug if diagnosis is confirmed by elevated pancreatic enzymes.