Case Presentation: A 58-year-old woman with a past medical history notable for thyroid cancer status-post thyroidectomy complicated by hypoparathyrodism presented with muscle spasms in her hands and feet for two days. Four days prior to admission she reported bloating and heartburn for which she reports taking an unknown quantity of lansoprazole and an H2 blocker. One day prior to admission she reported carpopedal spasms limiting her ability to grip objects, perioral tingling, and numbness in her distal extremities. She reported that the only other medications she took were calcitriol 0.5mcg and chlorthalidone 12.5mg daily. She reports that she was not taking calcium supplementation given recurrent nephrolithiasis. Her physical Exam was notable for a positive Chvostek and Trousseau signs but was otherwise unremarkable.
Her labs were notable for the Calcium 5.9 mg/dL (8.3-10.3mg/dL), Ionized Calcium 0.87mmol/L (1.11-1.30mmol/L), Mg 1.4 mg/dL (1.6-2.3mg/dL), Phosphorus 5.6 mg /dL (2.5-4.5mg/dL), parathyroid hormone 5 pg/mL (15-75pg/mL), and Vitamin D 25 16.8ng/mL (30-80ng/mL)
Her electrocardiogram was notable for a prolonged QTc of 484 ms.
Hospital Course:
The patient was successfully treated with of IV calcium gluconate, oral calcium carbonate and IV magnesium, with complete resolution of muscle spasms. Given the time course of her symptoms without any other interval events, her acute hypocalcemia was attributed to malabsorption from her recent PPI and H2 blocker use. She was advised to avoid these medications in the future.
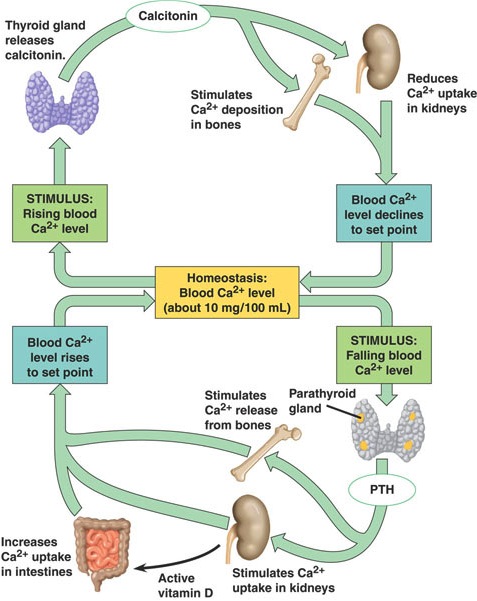
Discussion: Calcium homeostasis is regulated by the effects of parathyroid hormone (PTH) and vitamin D on the bones, GI tract and kidneys. The most common causes of hypocalcemia are iatrogenic hypoparathyroidism, vitamin D deficiency, and renal disease. This patient has a baseline iatrogenic hypoparathyroidism, with an acute triggering event of proton pump inhibitor (PPI) and H2 antagonist (H2RA )intake. PPIs (not H2RAs) have been associated with osteoporosis, osteoporotic fractures, and were thought to reduce fractional calcium absorption in women, though this finding has not been consistently replicated. More direct measures of intestinal calcium absorption with radio-labeled calcium have not shown long term effects from PPIs however no short term studies have been done.
Another possible PPI associated hypocalcemia pathway is through hypomagnesemia precipitated PTH inhibition. Several case series suggest that PPIs may lead to hypomagnesemia with a total of 13 such cases reported. Intestinal magnesium absorption can be impaired due the use of PPIs though the exact mechanism of this impairment has not been thoroughly studied. As this patient already had impaired PTH secretion to begin with, the loss of that remaining function may have tipped her over into negative calcium balance.
Conclusions: Short-term use of PPIs may precipitate acute hypocalcemia in patients with hypoparathyroidism through direct (reduced calcium absorption) or indirect (hypomagnesemia and PTH inhibition) pathways. In patients with low PTH, anti-acid use should be done cautiously.