Case Presentation: A 78-year-old female with dextrocardia presented to the hospital from her outpatient dermatologist for hypotension, hypoxia, and altered mental status. She became diaphoretic, dyspneic (SpO2 78%), and hypotensive with systolic blood pressure in the 80s after applying topical lidocaine for a microneedling procedure. Initial exam noted diaphoresis, diffuse facial erythema and flushing, orolabial swelling, and bilateral lower extremity edema. Labs revealed acute kidney injury (AKI), transaminitis, lactic acidosis, and elevated troponin. Chest x-ray noted diffuse pulmonary edema. Cardiac ultrasound showed reduced left ventricular ejection fraction (LVEF) and global hypokinesis. Cardiology performed a transthoracic echocardiogram (TTE) revealing a decreased LVEF (20%), global left ventricular hypokinesis, and apical ballooning consistent with Takotsubo stress cardiomyopathy. Tryptase was normal, reassuring against allergic reaction and anaphylaxis. The compounded topical lidocaine concentration was found to be 30% (23% lidocaine, 7% tetracaine, 2% phenylephrine), significantly above the maximum recommended 4% concentration. Toxicology was consulted for lidocaine overdose vs. local anesthetic systemic toxicity (LAST). Fortunately, her hospital course was uncomplicated, and she stabilized quickly. Her clinical picture was most consistent with lidocaine overdose given the high concentration of the topical lidocaine used and the absence of systemic toxicity signs (i.e. dysrhythmia, seizures). She was educated to avoid unnecessary or elective exposures to topical lidocaine and to ensure concentration never exceeds 4%. Guideline directed medical therapy for HFrEF was deferred to follow up. Follow up TTE showing recovered ejection fraction (55%) with normal biventricular function.
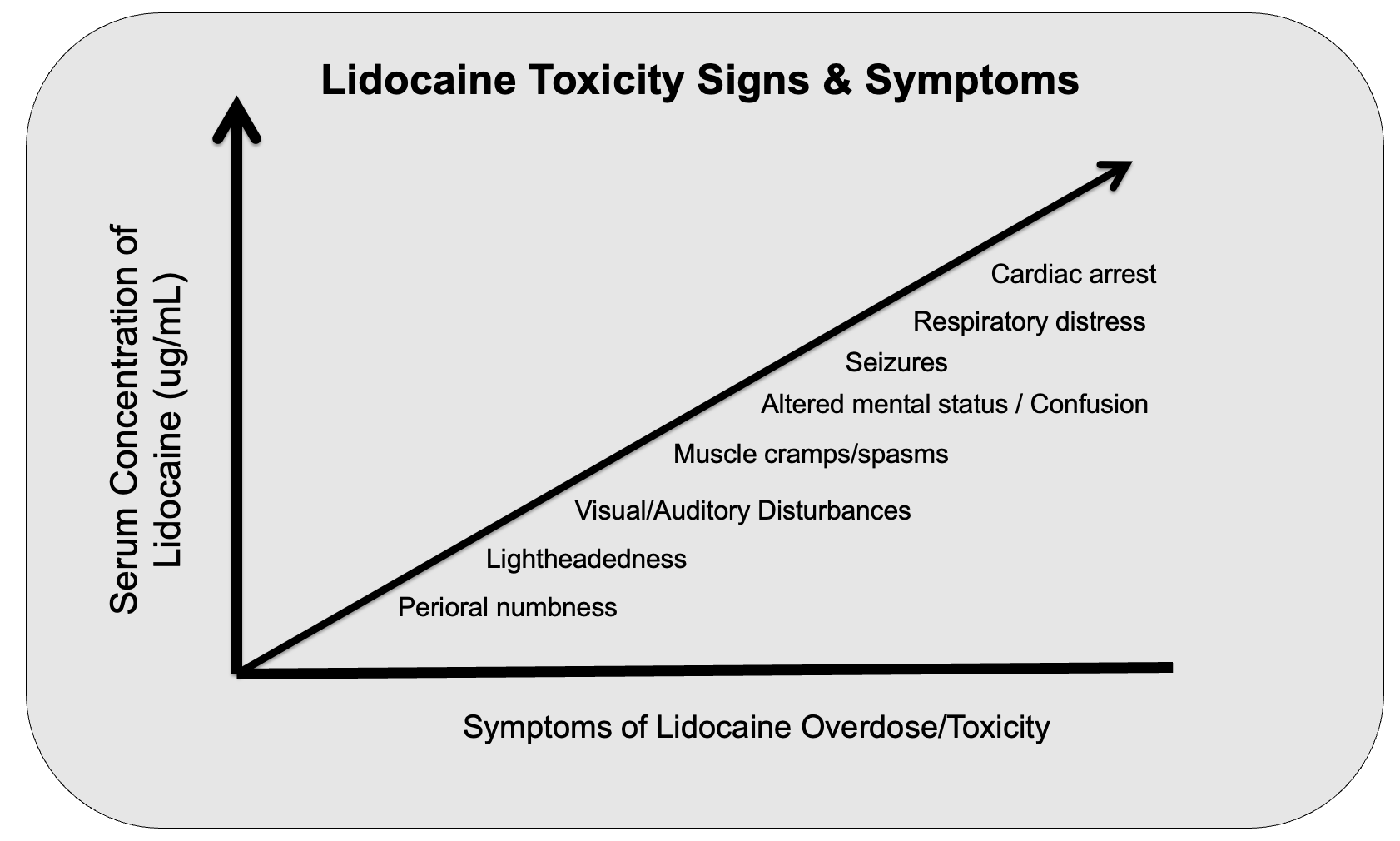
Discussion: Lidocaine overdose and LAST (local anesthetic systemic toxicity) are uncommon, particularly with topical formulations, but can result in fatal dysrhythmias, hemodynamic instability, & seizures due to inhibition of voltage gated sodium channels preventing initiation and propagation of action potentials. Overdose & toxicity are most associated with anesthetic-requiring interventions (i.e. surgery, injections, or nerve blocks), while toxicity from topical application is not frequently seen. Topical anesthetics are commonly used in outpatient dermatologic procedures (such as microneedling), as well as for other pain management scenarios.
Conclusions: Lidocaine overdose is uncommon but can result in acute cardiomyopathy and requires close in-hospital monitoring. Toxicity requires treatment with IV intralipid. Anesthetic overdose and toxicity are important to keep on the differential for hospitalized patients who become acutely altered or unstable, particularly those undergoing various procedural interventions, as diagnosis requires a fairly high level of suspicion and timely intervention.