Case Presentation: A 70-year-old man treated with Nivolumab for metastatic melanoma, presented with mild nausea and vomiting for a few days. He denied a change in urine output or appearance of urine, flank pain, or difficulty urinating. Creatinine on admission was 8.9 mg/dl (baseline 0.8mg/dl). Urinalysis revealed mild proteinuria, 21-50 WBCs/hpf. Spot protein/creatinine ratio was 0.52. C3 and C4 and CPK were normal. Renal ultrasound was unrevealing. He had no eosinophilia on his CBC with differential but had a few eosinophils in the urine. He was given fluid resuscitation overnight without improvement in creatinine. At that point, acute interstitial nephritis (AIN) due to Nivolumab therapy was suspected. He was treated empirically with high dose IV methylprednisolone 1 gram daily for three days. Over the next few days, his creatinine improved to 5.7 mg/dl. He was discharged home with a prednisone taper. Upon outpatient follow-up, his creatinine continued to improve close to his baseline.
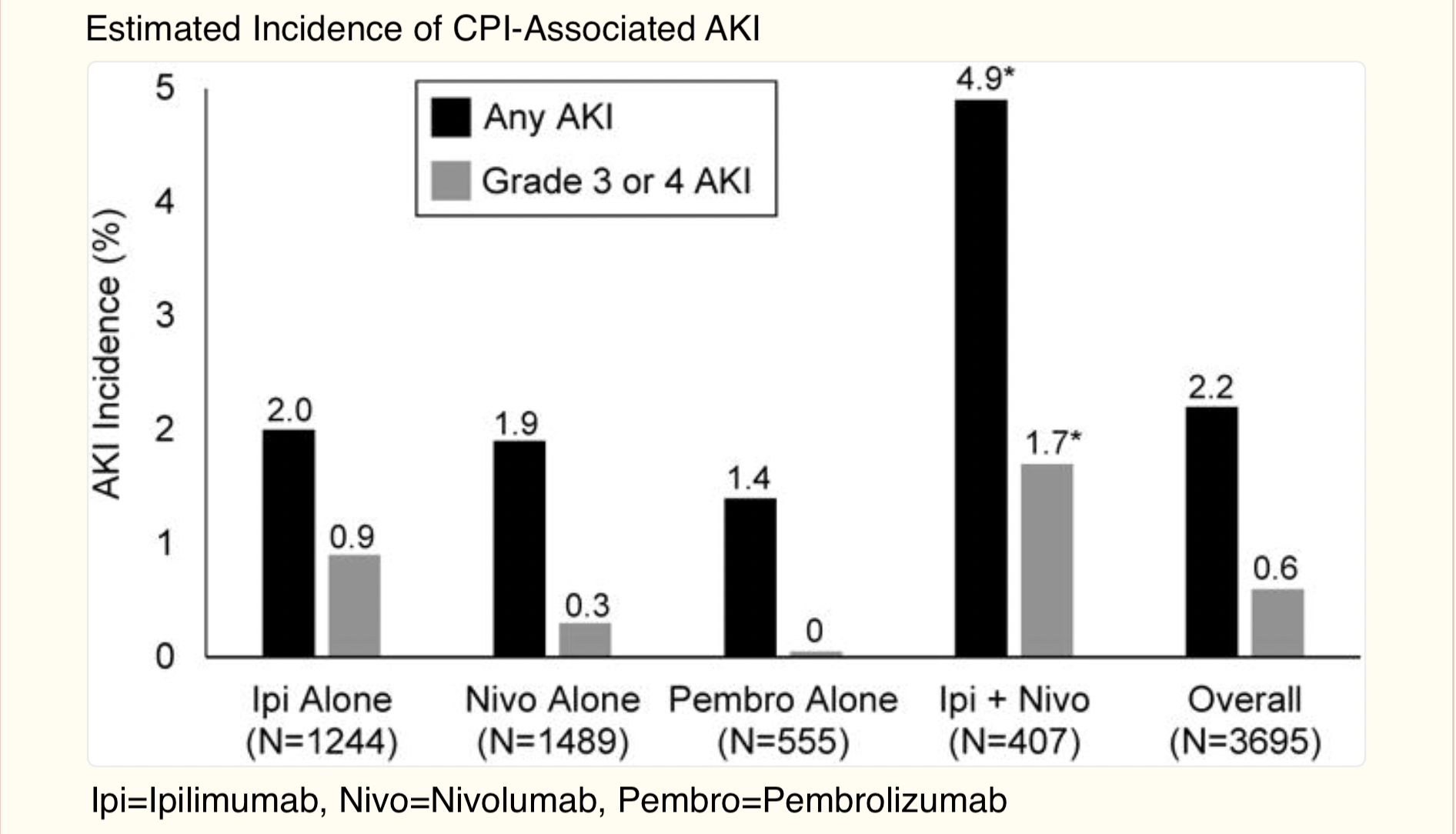
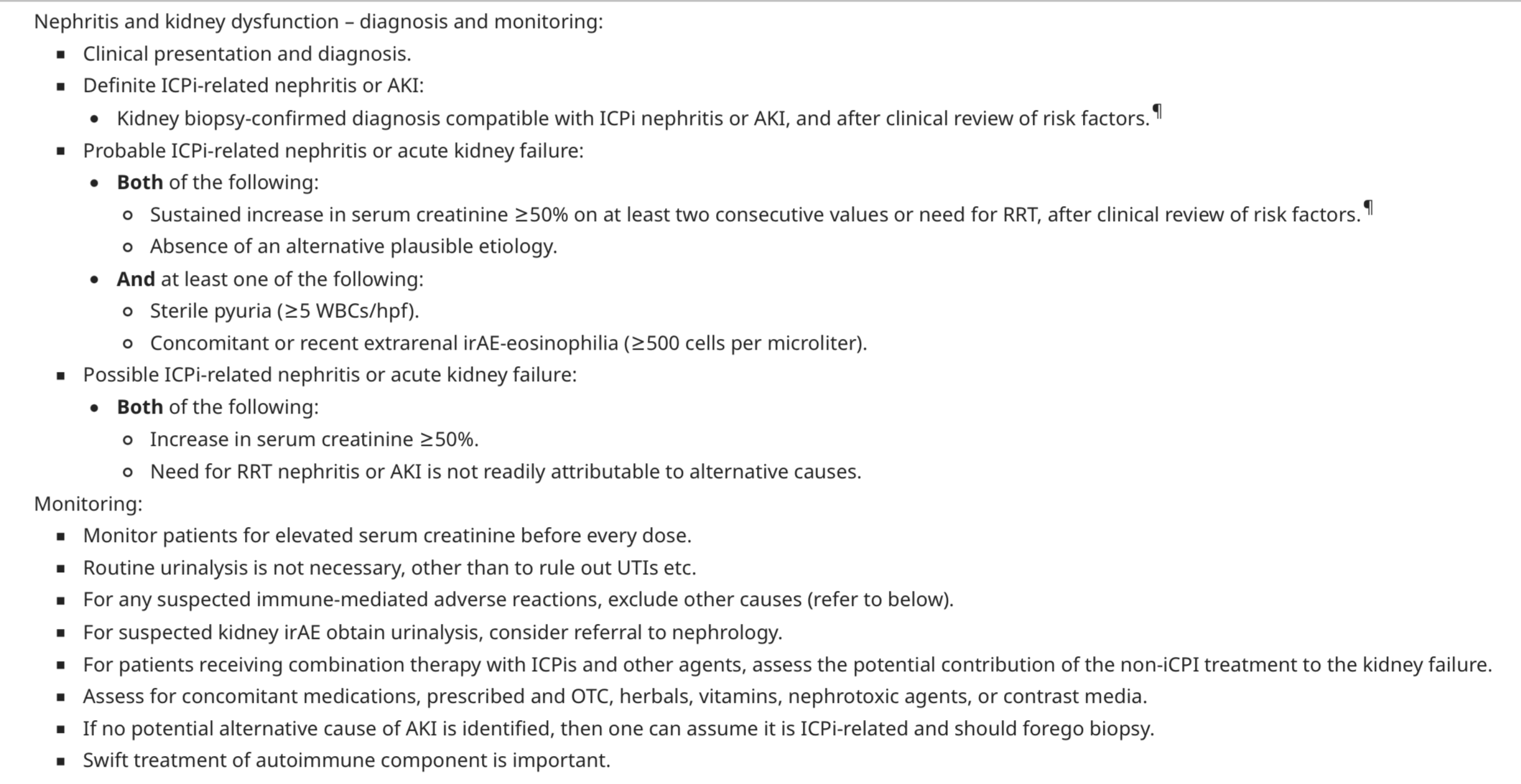
Discussion: Nivolumab, an immune check point inhibitor (ICPi) is a fully human immunoglobulin G4 (IgG4) monoclonal antibody that selectively inhibits programmed cell death-1 (PD-1) activity by binding to the PD-1 receptor to block the ligands PD-L1 and PD-L2 from binding. The negative PD-1 receptor signaling that regulates T-cell activation and proliferation is therefore disrupted. This releases PD-1 pathway-mediated inhibition of the immune response, including the antitumor immune response. T-cells can turn against a person’s own tissues, resulting in immune-related adverse events (irAE) that can affect almost any organ. We present a case of AIN induced by Nivolumab. ICPi therapy is associated with an increased risk of irAEs in melanoma patients; however, severe renal complications are still rare (See graph). AIN should be suspected in a patient with an elevated serum creatinine and a urinalysis that shows white cells, white cell casts and eosinophiluria. Drug-induced AIN should be suspected in the context of characteristic laboratory findings that can be attributed to a drug that has been previously reported to cause AIN. Kidney biopsy can be considered but it is not necessary for the diagnosis if the patient has acute kidney injury and greater than 5 WBCs/hpf in the urine in the absence of an alternative cause as was the case in our patient (See table). There are a limited number of case reports for Nivolumab-associated AIN. It can occur after weeks or months of therapy. Risk is increased with preexisting chronic kidney disease and concomitant use of agents that can cause AIN. Prompt response to treatment with steroids as we saw in our patient supports the diagnosis. It is unknown whether a checkpoint inhibitor (CPI) should be resumed after an episode of AIN. There have been reports of recurrence with resumption of CPI therapy. There are no established guidelines for the duration of steroid therapy. Generally, a prednisone taper of 3 months has been reported to be successful.
Conclusions: Although CPI agents are mostly considered non-nephrotoxic, this case report highlights a rare side effect of Nivolumab as AIN. Close monitoring of renal function and electrolyte disturbance is crucial for early recognition of renal toxicities in patients receiving CPI therapy. Remember that friendly fire can happen due to ICPi and any patient getting hospitalized who is on a ICPi should be evaluated for the possibility of irAE. We advocate for patients on ICPi to carry a card delineating their treatment and possible toxicities.