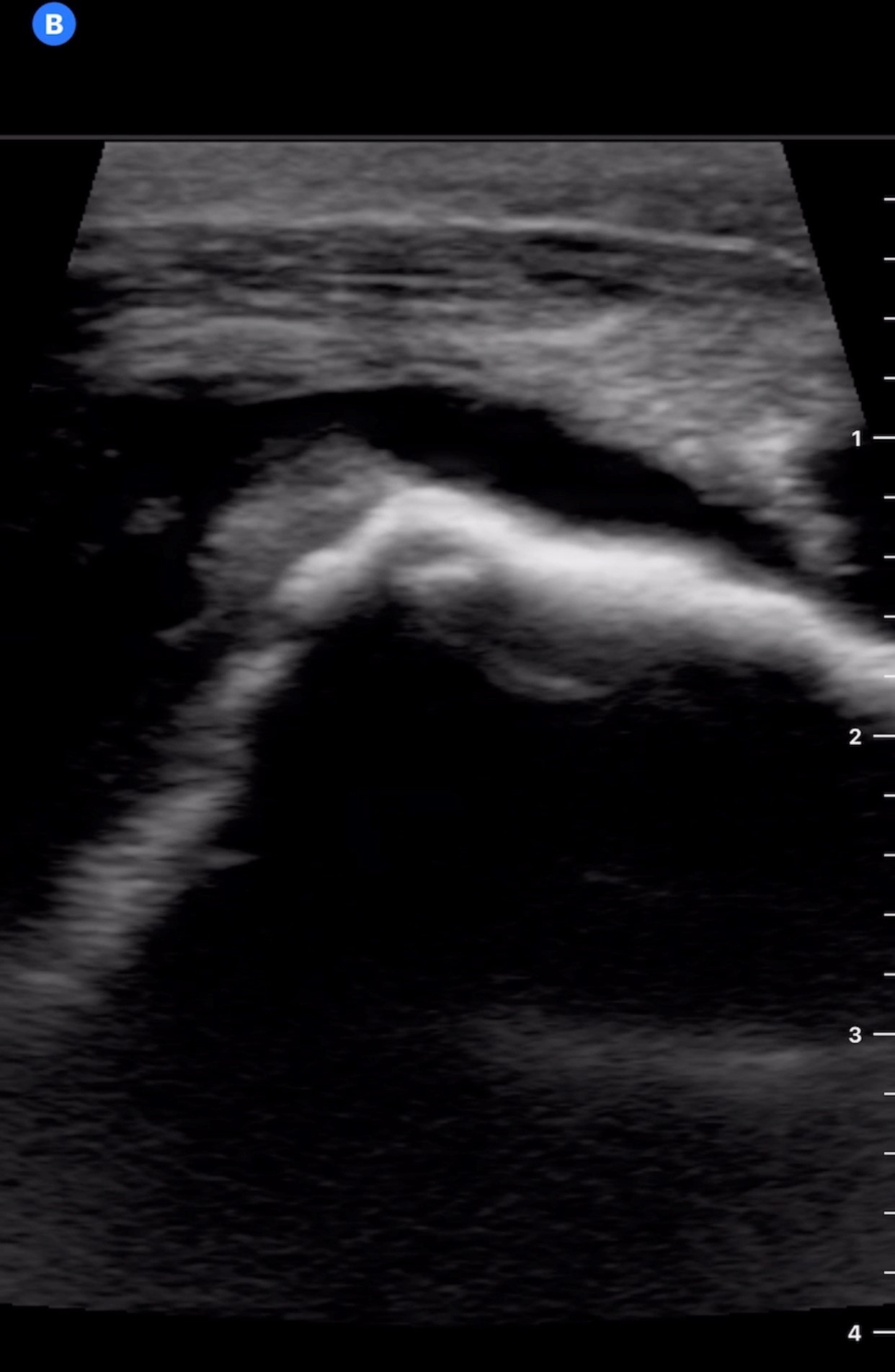
Case Presentation: A 73 year-old woman with a history of recurrent pancreatitis, severe osteoarthritis presented to the ED with acute pancreatitis. On hospital day 3 she noted right shoulder pain, similar to her chronic arthritis but worse in intensity. Her examination did not reveal any abnormalities; she had severely limited ROM of motion due to pain. She was given her home opioids without relief. Overnight she became febrile to 101.7°F. The next morning her shoulder pain was significantly worse and she noted pain of her right elbow. Examination revealed a swollen right elbow with overlying warmth and no erythema, along with tenderness of the right shoulder. A bedside point-of-care ultrasound (POCUS) revealed a right shoulder and elbow effusion. Arthrocentesis of the right elbow was performed. The synovial fluid cell count was >100,000 cells/mL (0-200 cells/mL), of which 97% were neutrophils. Gram stain was unremarkable and positively birefringent calcium pyrophosphate (CPP) crystals were noted. Her ESR was 70 mm/hr (0-30 mm/hr), CRP 171 mg/L (0.0-10.0mg/L), and she had a peripheral leukocytosis of 12,300 cells/mL (4,5000-11,500 cells/mL). Her clinical picture initially raised concern for septic arthritis, but the synovial fluid analysis suggested calcium pyrophosphate deposition disease (CPPD). She was placed on colchicine. Subsequently, she developed synovitis of her right wrist, DIP, and PIP joints. The migratory and progressive joint involvement was unusual for CPPD and high-grade fevers continued to be worrisome for septic arthritis. Blood and fluid cultures did not yield any growth. Gonococcal and HIV testing were negative. Steroid therapy was added. By hospital day 6, she had significant improvement in her pain and swelling and remained afebrile. She was ultimately discharged home in stable condition with a treatment course for CPPD.
Discussion: CPPD is the third most common inflammatory arthritis. It typically presents as acute mono- or oligoarthritis. It is often associated with underlying osteoarthritis. Acute disease flares can occur with underlying acute illnesses, including pancreatitis. Diagnosis is made by clinical presentation, imaging, and synovial fluid analysis. Synovial fluid characteristically reveals weakly positively birefringent CPP crystals detected by light microscopy. CPP crystals and polymorphonuclear leukocytes are virtually always present in inflamed joints during an acute attack. The total synovial fluid leukocyte concentration is typically 15,000-30,000 cells/mL, with up to 90% neutrophil predominance. The presence of atypical features (migratory polyarthritis, systemic inflammation, markedly elevated synovial fluid cell count) should raise the diagnostic suspicion of alternate etiologies given their rare occurrence with CPPD. . Suspicion for septic arthritis should remain high in this type of clinical presentation. Alternately, conditions such as gout, pseudogout, rheumatoid arthritis may be potential causes of pseudoseptic arthritis and should be considered in patients with underlying inflammatory disorders that present with acute arthropathy with systemic signs and symptoms.
Conclusions: Migratory arthritis, high-grade fever and systemic inflammatory responses are uncommon in CPPD. Their presence should raise suspicion for alternate diagnoses, particularly infection. Confirming diagnosis by synovial fluid analysis and recognizing atypical presentations of common diseases are essential to ensure appropriate clinical care.