Background: A somewhat under-discussed topic in EHR implementation is the safety and efficiency consequences of their lengthy build and implementation. After multiple years of stalled clinical innovation while IT staff dedicate their focus to EHR builds, hospital systems undergo an 8 – 16 hour downtime often followed by multiple planned and unplanned downtimes that can cause a multitude of patient safety issues due to the lack of access to lab orders and reports(1, 2).
1. Sittig, D, et al. Safe EHR Use Requires a Comprehensive Monitoring and Evaluation Framework. JAMA. 2010;303(5):450-451.
2. Larsen, E, et al. Implications of EHR downtime: an analysis of patient safety event reports. JAMIA. 2018;25(2):187–191.
Purpose: We created a web-based tool used for rounding and team-based task management that auto-populates data, generates tasks, can be edited by multiple users simultaneously, and is accessible via computer and phone that is used across 130 services and 4 hospitals. Though the initial purpose of this tool wasn’t dedicated towards solving the issue of data availability during downtime, we reviewed data usage during downtime to determine whether workspace tools have the potential to patch the discontinuity that occurred during go live.
Description: Six months after we installed our workspace tool, our institution implemented a new EHR, during which there were a total of 27 hours of downtime across 4 hospitals spread across two days. We reviewed available usage data as well as intra-app actions to assess how this application was utilized during the downtime. During the downtime, the tool allowed clinicians to retain access to vital patient information, including care team assignments, vital signs, labs, medications, clinical care plans, and tasks. It continued to pull in clinical data from the old EHR, which was otherwise in a “read only” view that didn’t integrate with the new EHR. Clinicians could take notes, update tasks, and ultimately import them into the new EHR. Users reported feeling much less anxious about accessing and finding clinical data than they had anticipated because they knew they could find it within our tool quickly.
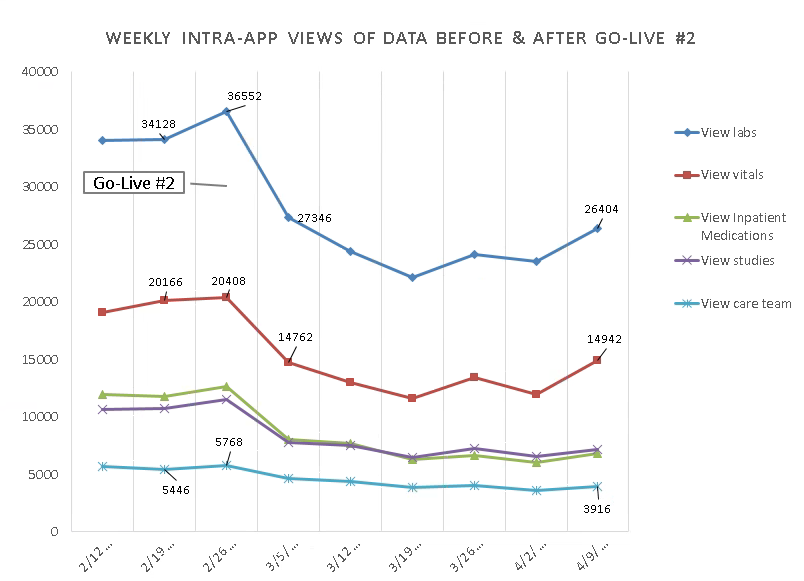
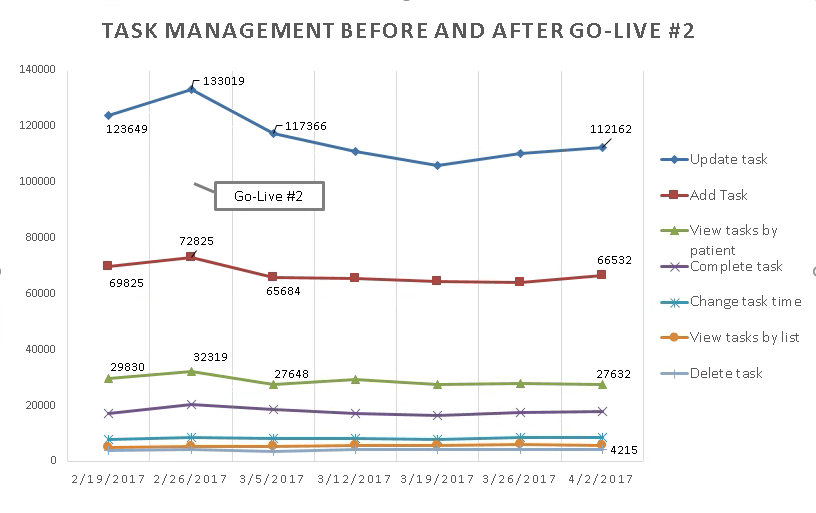
Figures 1 & 2 demonstrate that during our EHR implementation, users accessed our application to view clinical data and manage their tasks more frequently than on weeks prior to the go-live. While there was a decrease after go-live, user activity ultimately leveled out. Interestingly, while users continue to view data in the application, that usage has decreased more significantly than task management, likely because there are now additional data visualization options with the new EHR.
Conclusions: It is critical to think of how we can preserve safe patient care during EHR downtime, especially as EHRs become increasingly available across hospital systems. We describe a novel approach to improving patient safety, efficiency and clinician experience during downtime by utilizing an interoperable application that has the capacity to populate clinical data and care planning information to retain institutional memory when transitioning EHRs.