Background: Hospitalization frequently leads to functional decline in older adults due to immobility, acute illness, and iatrogenic factors. Nutritional status often deteriorates concurrently because of reduced appetite, restrictive diets, and physical barriers. Together, deconditioning and malnutrition increase morbidity, prolong hospital stay, and raise readmission risk. This project evaluated the impact of structured early mobility interventions on functional status and explored the relationship between mobility and nutritional intake. We theorized that early mobilization combined with targeted nutritional support would reduce acquired weakness, enhance functional independence, and improve nutritional outcomes in hospitalized older adults.
Purpose: To employ early mobilization and nutritional support to preserve or improve functional independence, mitigate hospital associated deconditioning and improve care quality for older adults.
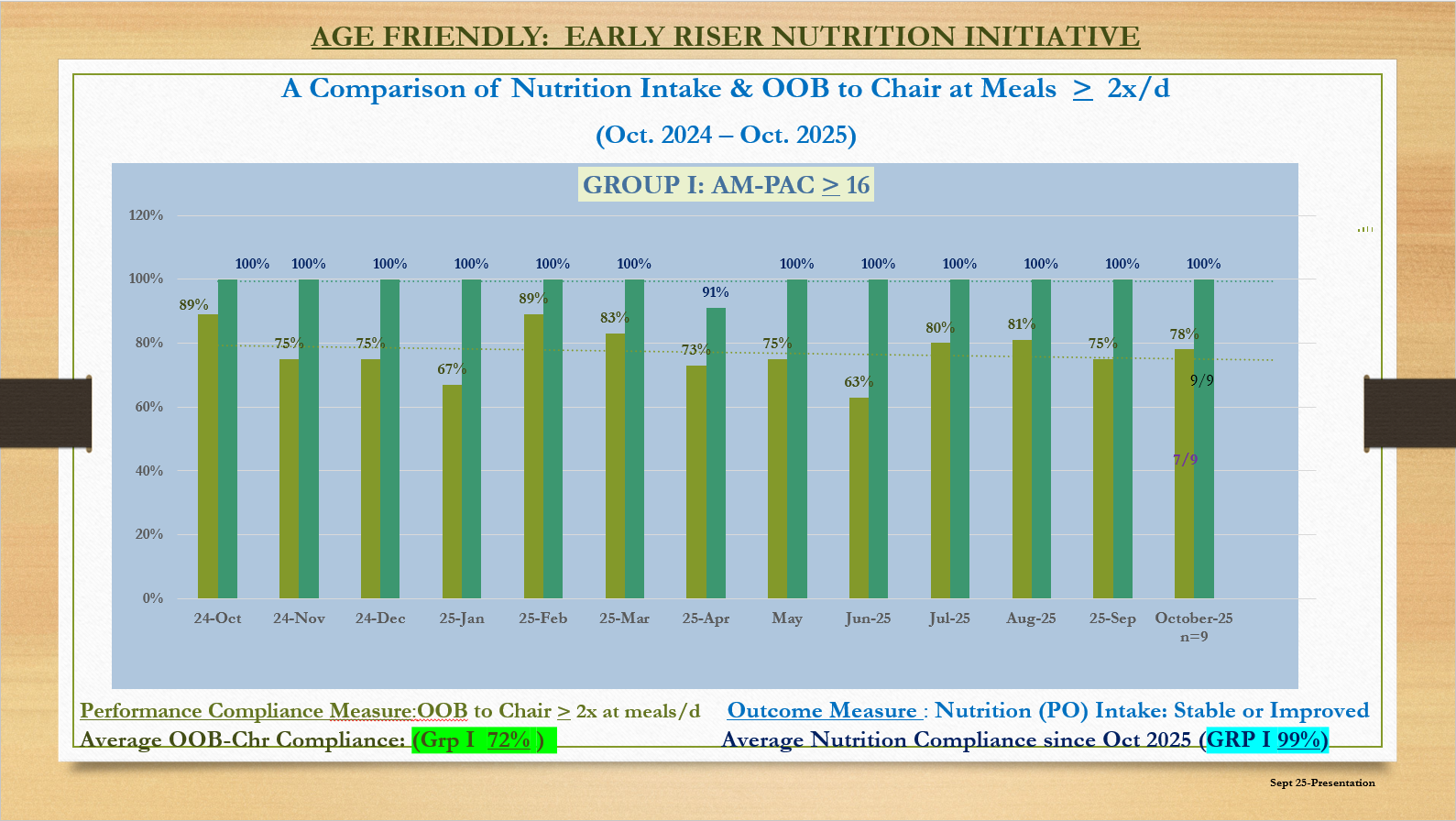
Description: As an Age-Friendly Health System, we employ 4M framework in our interdisciplinary rounds. Since mobility is a key component of 4M methodology, We utilize the AM-PAC 6-Clicks tool to assess functional status of all admitted patients. Assessment occurs within 24 hours of admission and at regular intervals during their hospital course. Scores are reviewed daily to identify patients at risk for mobility decline. Using this data, we initiated an “Early Rise” program where staff identified patients with scores of 12–16 (requiring more assistance and supervision during ambulation) and those with scores of 17–24 (independent or requiring minimal assistance). With the help of staff, patients received twice-daily 10-15 minutes ambulation sessions. A nutrition-focused initiative was layered onto this mobility program to assess and optimize the relationship between patient mobility and nutritional intake. Patients with AM-PAC 6-Clicks scores of 17 or greater were selected for the pilot. The staff ensured that at least two meals per day were consumed out of bed in a chair, leveraging evidence that upright positioning and communal dining improve meal intake and nutritional status in hospitalized older adults. Registered dietitians collaborated with nursing to monitor and quantify meal/tray completion. Meal intake was categorized as follows: 75-100% (good), 50-74% (fair), 25-49% (poor), and less than 25% (very poor). Dietitians performed nutrition assessments and ensured that care plans were implemented as prescribed. Standardized outcome indicators included percentage of meal completion and functional status, with regular documentation and quality improvement review.Adding the nutritional component to the Early Rise program demonstrated that upright meal consumption was strongly associated with higher meal completion (75–100%), indicating improved intake. Patients reported greater satisfaction, citing enhanced comfort and appetite when eating in a chair. These initial results are encouraging, and future plans include expanding the program to patients with AM-PAC 6-Clicks scores of 12–16 to further enhance care quality for older adults.
Conclusions: Integrating early mobility with structured nutritional support significantly improved functional recovery, nutritional intake, and patient satisfaction. This novel combined mobility-nutrition initiative represents a scalable, multidisciplinary, age-friendly approach to preventing hospital-associated deconditioning and malnutrition in older adults.