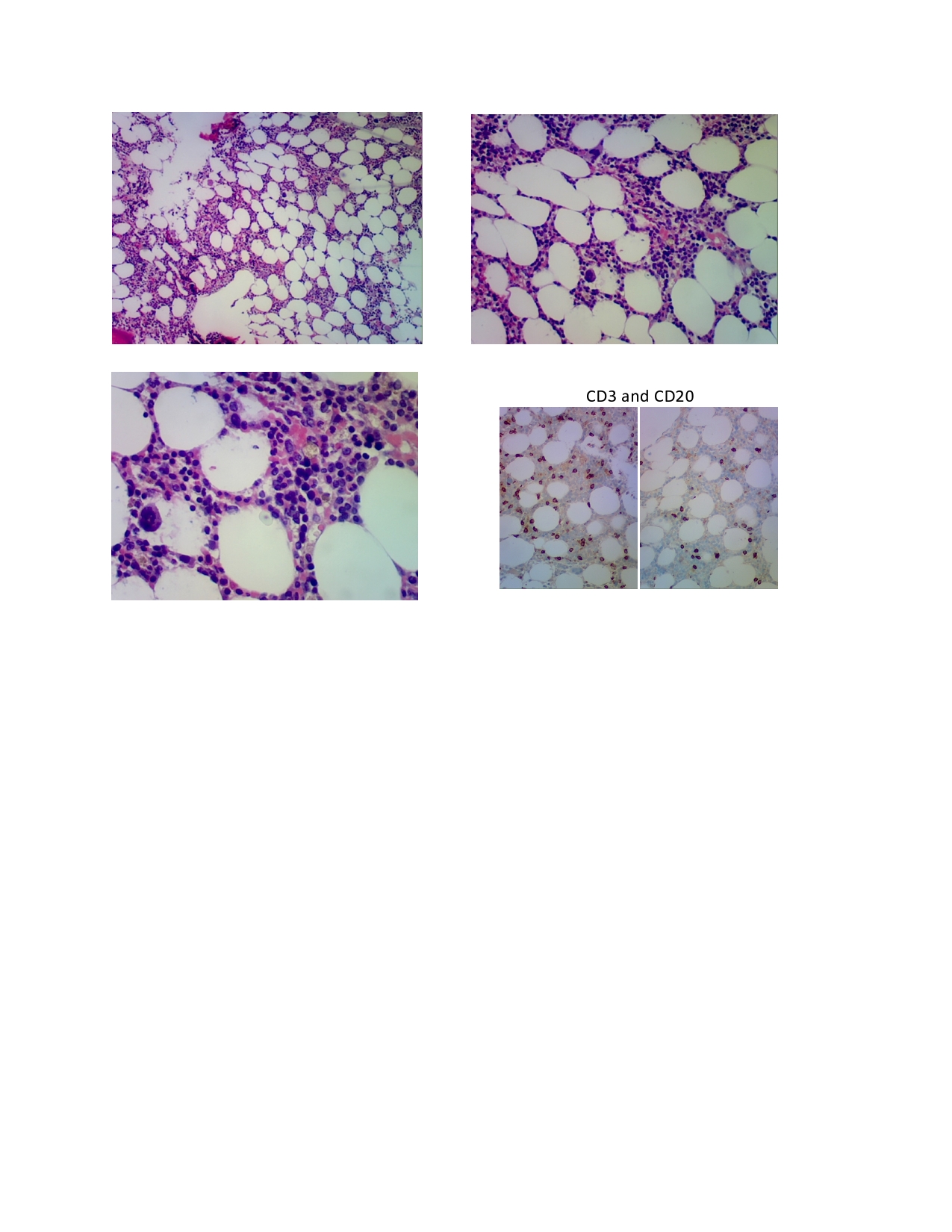
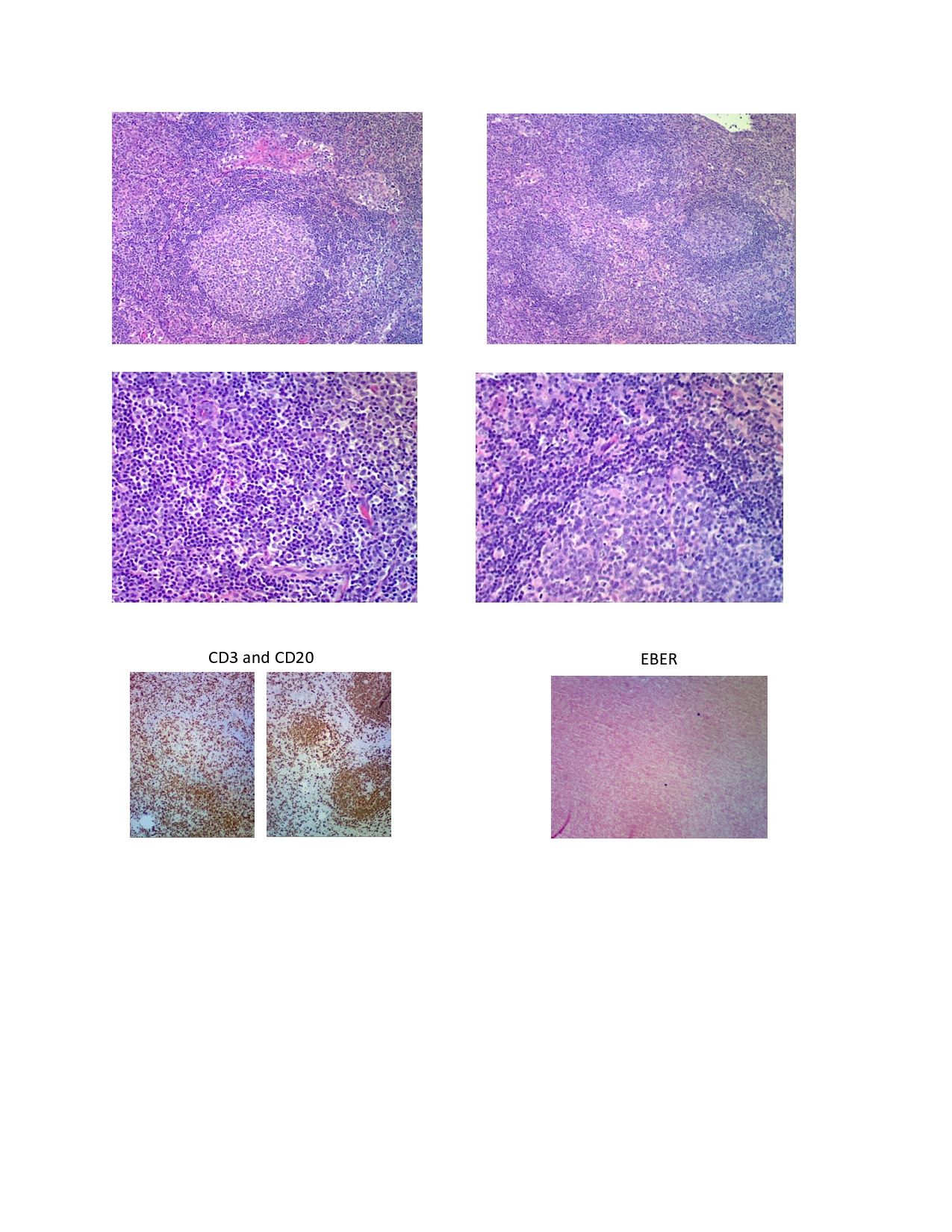
Case Presentation: A 29-year-old male presented to our hospital with four weeks of worsening fatigue, shortness of breath and a 15lb weight loss due to anorexia. He was short of breath walking up a single flight of stairs, which resolved with rest. He had no environmental exposures, sick contacts or recent travel. His mother had a history of sarcoidosis. He was seen 3 weeks earlier for similar symptoms and was found to have bilateral axillary and retropectoral lymphadenopathy on chest CT. Initial physical exam noted bilateral axillary lymphadenopathy. The remainder of the physical exam was benign, with no hepatosplenomegaly and no erythema or exudates of the mouth and pharynx.Initial laboratory investigations upon admission revealed leukocytes of 2.3 x103. The leukocyte differential count showed segmented neutrophils 43% and lymphocytes 56%. Hepatic panel was significant for AST 205 U/L, ALT 143 U/L, and an albumin 2.5 g/dL. Blood cultures were negative. An extensive laboratory work-up for infectious and rheumatologic markers was also benign, including negative mononucleosis heterophile antibody and EBV-VCA antibodies IgM. EBV-VCA antibodies IgG and EBV IgG antibodies to nuclear antigen were positive. This picture looked negative for acute infection with EBV. A malignant process was considered. A left excisional axial lymph node biopsy showed a benign reactive process with follicular hyperplasia, paracortical hyperplasia and focal dermatopathic changes. A subsequent bone marrow biopsy showed overall hypocellularity with only 25% of the marrow being cellular without evidence of infectious agents or dysplasia.
An EBV DNA qualitative PCR analysis was performed and was positive for EBV DNA. The patient had improvement clinically and in laboratory values with supportive care.
Discussion: Epstein-Barr virus (EBV) is the most common cause of infectious mononucleosis (IM) with incidence rate of 90% of all cases. The classic syndrome of IM includes sore throat, headache, anorexia, fatigue and low-grade fever. However, EBV has different ways of presenting and may imitate other infections or malignancies. EBV has oncogenic properties and is associated with multiple malignancies in both immunocompetent and immunocompromised individuals.
EBV infects 90-95% of adults worldwide. In most cases, symptoms spontaneously resolve within 2 to 3 weeks but fatigue may persist for months or even indefinitely.
Heterophile antibodies are not specific and remain negative in some patients. EBV-specific antibody profiles and EBV DNA PCR are the best choice for staging EBV infection when the suspicion of IM is high. Furthermore, following EBV viral loads may help in the detection of EBV-associated malignancies in immunosuppressed patients.
This case report highlights the importance of EBV PCR in making the diagnosis of atypical presentation of EBV infection when negative EBV serologies mislead the diagnosis, and emphasizes that EBV infection may mimic lymphoma.
Conclusions: This case report highlights the importance of EBV PCR in making the diagnosis of atypical presentation of EBV infection when negative EBV serologies mislead the diagnosis, and emphasizes that EBV infection may mimic lymphoma.