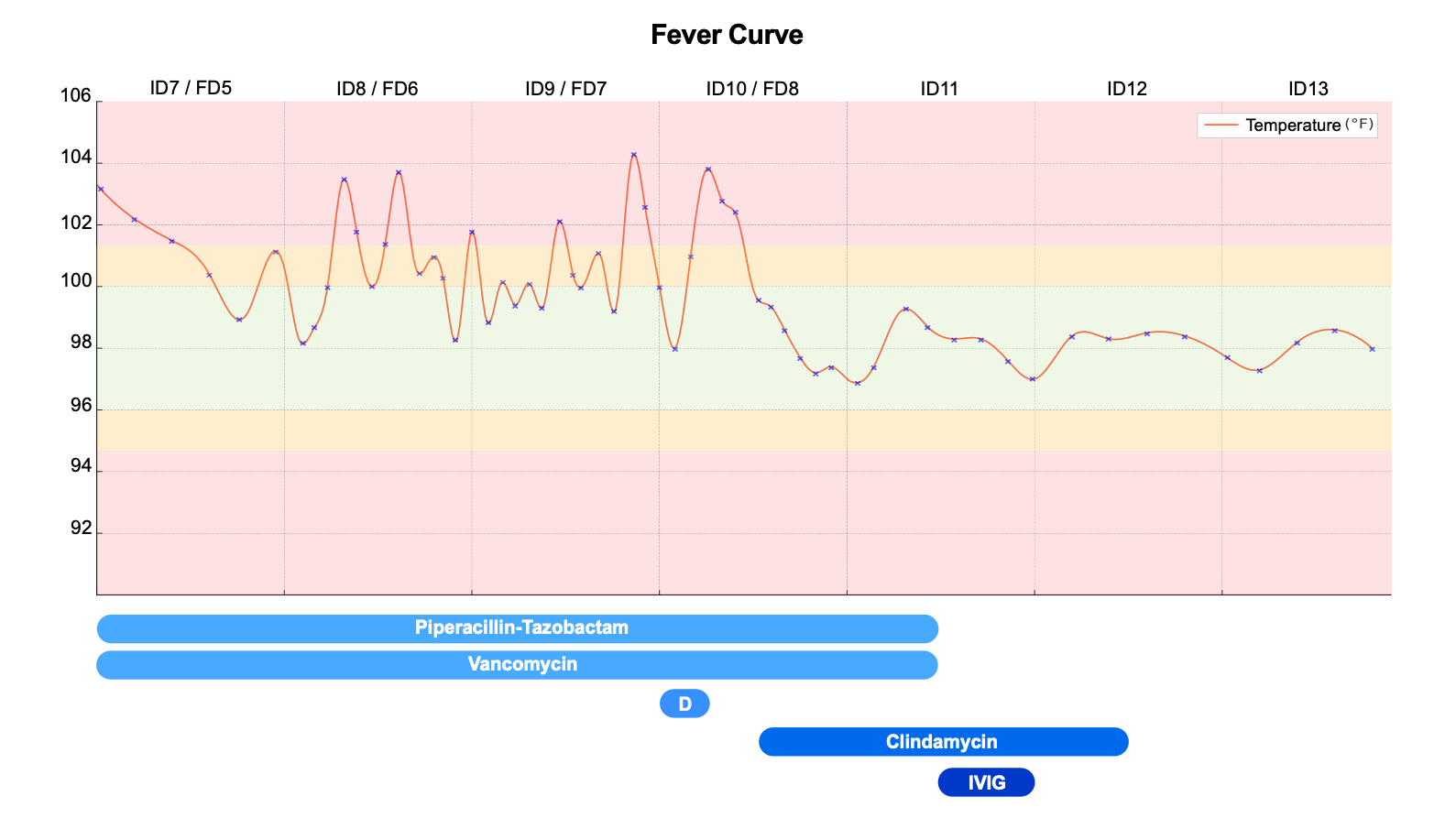
Case Presentation: A previously healthy 4-year-old male initially presented with lower abdominal pain. Abdominal and pelvic CT showed mild left external iliac and inguinal lymphadenopathy. The next day, he developed a low-grade fever and an erythematous patch over the left groin. He was diagnosed with cellulitis and oral trimethoprim-sulfamethoxazole was initiated. He re-presented 24 hours later with worsening rash, leukocytosis, and an elevated C-reactive protein (CRP). He was started on IV clindamycin, ampicillin-sulbactam, and oral azithromycin. New findings included dry, cracked lips; a pinpoint erythematous rash; bilateral conjunctival injection. Rapid progression of the erythema along with systemic signs raised concern for a necrotizing soft tissue infection prompting initiation of piperacillin-tazobactam and vancomycin. Fever persisted despite broad-spectrum antibiotics, and advanced imaging was negative for fasciitis. Conjunctivitis and rash progressed, raising concern for incomplete KD, which was supported by laboratory criteria. Intravenous immunoglobulin and moderate-dose aspirin were administered and antibiotics were discontinued. The patient defervesced, skin findings improved, and CRP decreased to normal range.
Discussion: Kawasaki disease can present in a number of ways outside of the typical manifestations, ranging from pancreatitis to torticollis. These atypical presentations pose a challenge to the diagnosis and ultimately can delay the proper management of Kawasaki disease. Pulmonary (e.g., infiltrates, respiratory distress) and gastrointestinal (e.g., vomiting, abdominal pain, pancreatitis) manifestations were the most frequently found atypical features. Cutaneous manifestations other than the typical rash include those that are scarlatiniform, erythema multiforme-like, urticarial, pustular, or psoriatic. When severe, the rash, conjunctivitis, and oropharyngeal manifestations could be mistaken for Stevens-Johnson Syndrome.Cutaneous manifestations beyond the typical rash are rare, although the prevalence has not been reported in the literature. To our knowledge, ours is the third report of KD presenting with inguinal cellulitis. Similar to the prior reports, in our case, there was high suspicion for cellulitis because the patient had localized warmth, tenderness, and swelling of the inguinal region associated with fevers. The initial rapid spread of erythema also raised concern for necrotizing fasciitis that was not confirmed on CT or MRI imaging. Only on day 6 after initial symptoms did a patchy, macular, erythematous rash erupt similar to skin findings more commonly found in KD. Our patient’s clinical manifestations improved rapidly after IVIG administration, with complete resolution at a 2-week follow-up visit.
Conclusions: Early detection of Kawasaki disease is important in patients as prompt treatment impacts clinical outcomes. IVIG should be started within 10 days of fever onset to decrease the risk of coronary aneurysm. In our patient, the differential was broadened after no improvement on broad-spectrum antibiotics, and Kawasaki disease was considered. This case highlights the importance of considering Kawasaki disease for a patient presenting with a localized rash, several days of fevers, and laboratory abnormalities for the appropriate treatment to be initiated.