Background: Immobility in hospitalized patients remains prevalent, leading to multiple hospital acquired complications including pressure injuries, venous thromboemboli, and falls. In our large tertiary care, academic hospital we piloted an innovative interprofessional education course which demonstrated health professional students could mobilize inpatients without increasing falls. Our initial promising results led to an expansion of the student cohort, and we hypothesized that student mobilizers would decrease immobility harm compared to usual care.
Purpose: To evaluate the effect of an innovative, interprofessional mobility curriculum on inpatient immobility harm.
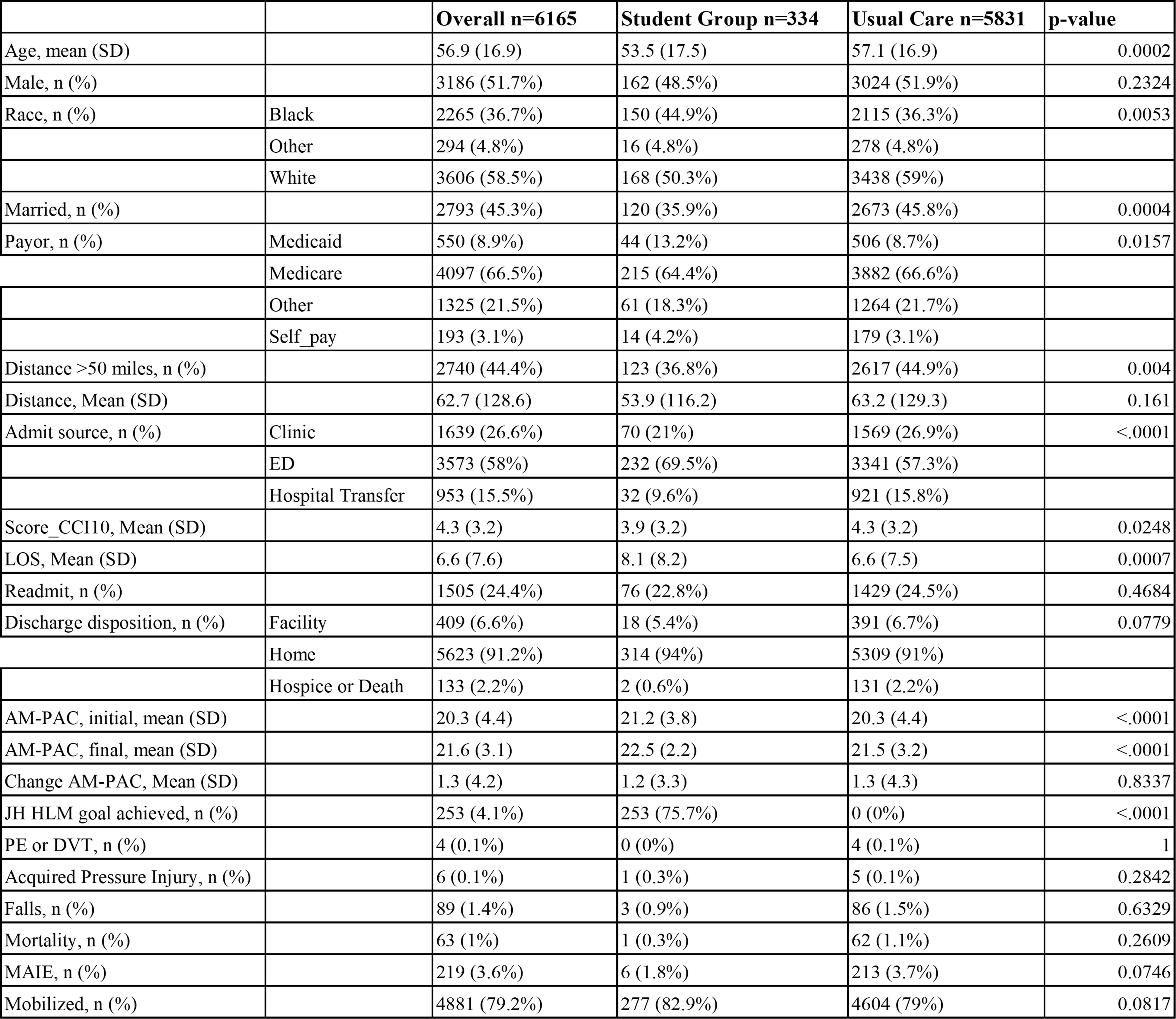
Description: Our mobility course was offered to all health professional students across campus. The course consisted of one lecture by a physician reviewing literature on mobility, followed by a demonstration of interprofessional communication and appropriate mobilization techniques for ambulatory inpatients by a physical therapist (PT). PT evaluated the students to ensure correct performance of patient mobilization. Thereafter, students independently mobilized hospitalized patients with nursing evaluated Activity Measure for Post Acute Care (AM-PAC) score >17, indicating the patient is ambulatory. We performed an analysis comparing the Student Group (SG) – individual patient hospitalizations during which a student attempted to mobilize the patient at least once – to usual care (UC) – patient hospitalizations on the target units that the students did not attempt to mobilize. Our primary outcome was Major Adverse Immobility Events (MAIE), which we defined as hospital acquired venous thromboembolism, pressure injury, falls, or all-cause mortality. The patients our interprofessional students attempted to mobilize showed a trend towards a lower MAIE – SG 1.8% (6/334) vs UC 3.7% (213/5831), though it did not reach statistical significance. Our secondary outcomes were documented mobilizations and falls. The Student Group also showed a trend towards more mobilizations – SG 82.9% (277/334) vs UC 79% (4604/5831) and fewer falls – SG 0.9% (3/334) vs UC 1.5% (86/5831), though neither reached statistical significance. Table 1 further details the demographics and outcomes for the intervention and control group.
Conclusions: Our innovative interprofessional curriculum showed a trend towards improvement in immobility harm and increased mobilization of patients with fewer falls. Our study is limited by introduction of bias because we did not randomize the patients mobilized by students. This can be seen in the minor differences in groups in Table 1, for example, the SG including younger patients and more African American patients. It is possible our intervention group is not sufficiently powered to demonstrate statistical significance, and we plan to continue to analyze as more students mobilize patients. Our study can be replicated at other academic institutions as it required low effort, carried minimal associated risks, yet had potential for high impact.