Background: A recent uptick in hospital readmissions, prolonged lengths of stay that was above national benchmarks, and declining patient satisfaction scores threatened the institution’s reputation within the community and risked CMS reimbursement penalties. In response, an interdisciplinary physician-led huddle followed by a structured nurse-physician bedside rounding protocol was developed. This approach was designed to strengthen communication, enhance patient experiences, and optimize hospital throughput. This intervention was initially piloted on a 46-bed medical-surgical unit in a small community hospital.
Purpose: The primary aim of this initiative was to foster a cohesive interdisciplinary team dynamic, proactively discuss patient care plans, and conduct RN/MD bedside rounding. This approach integrates the team’s efforts to enhance patient care, improve communication, and streamline discharge planning, ultimately reducing the reliance on Epic secure chats that contributed to provider burnout, alarm fatigue, and delays in urgent communication. The trial aimed to reduce readmissions, minimize extended lengths of stay, enhance hospital throughput, and elevate patient satisfaction scores.
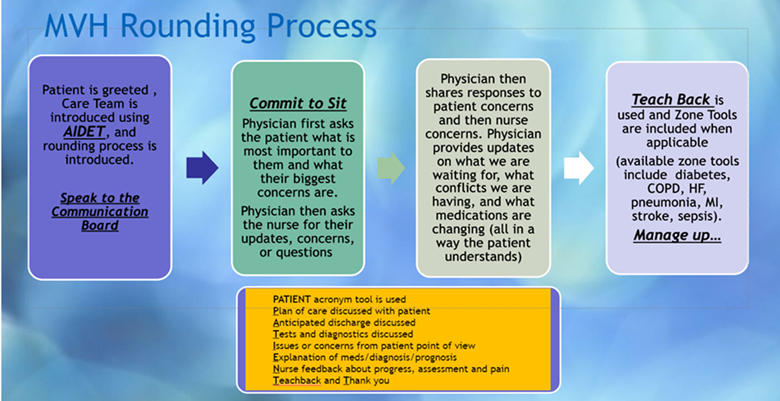
Description: The first step involved aligning nursing assignments with physicians’ geographic locations within the hospital for better efficiency. Physicians were strategically positioned, with assigned time slots for efficient huddle management. The interdisciplinary team included nurse managers, bedside nurses, social workers, care managers, pharmacists, home health representatives, nurse practitioners, physical and occupational therapists, and dietitians. Each day, team members received an assignment checklist detailing roles and responsibilities for huddle participation. The design emphasized proactive care plan discussions followed by RN/MD bedside rounding. This patient-centered rounding model fostered direct communication between the nurse, physician, and patient, centering the conversation at the bedside to keep the patient fully informed. Weekly stakeholder meetings allowed the team to review outcomes, identify improvement opportunities, and refine strategies based on feedback. Summaries and goals for the coming week were provided via follow-up emails to maintain focus and alignment.
Conclusions: Standardizing the morning interdisciplinary huddle has improved communication, streamlined discharge planning, and positively impacted on HCAHPS scores, particularly in physician communication, Anecdotal feedback indicated a reduction in Epic secure chats, which decreased interruptions and improved team workflow. The Care Transitions domain improved by 23.7% compared to pre-trial scores, reflecting those patients felt better supported in medication management, follow-up appointments, and their understanding of their condition post-discharge.Positive impacts on throughput and length of stay were also noted, with discharges before 11 AM increasing pre-trail from 14.8% to 25.9% post-trial. Overall, this initiative has fostered patient-centered care, enhanced team communication, and created a more efficient rounding process. Ongoing data analysis will continue to measure the long-term effects of this initiative on operational efficiency and patient outcomes