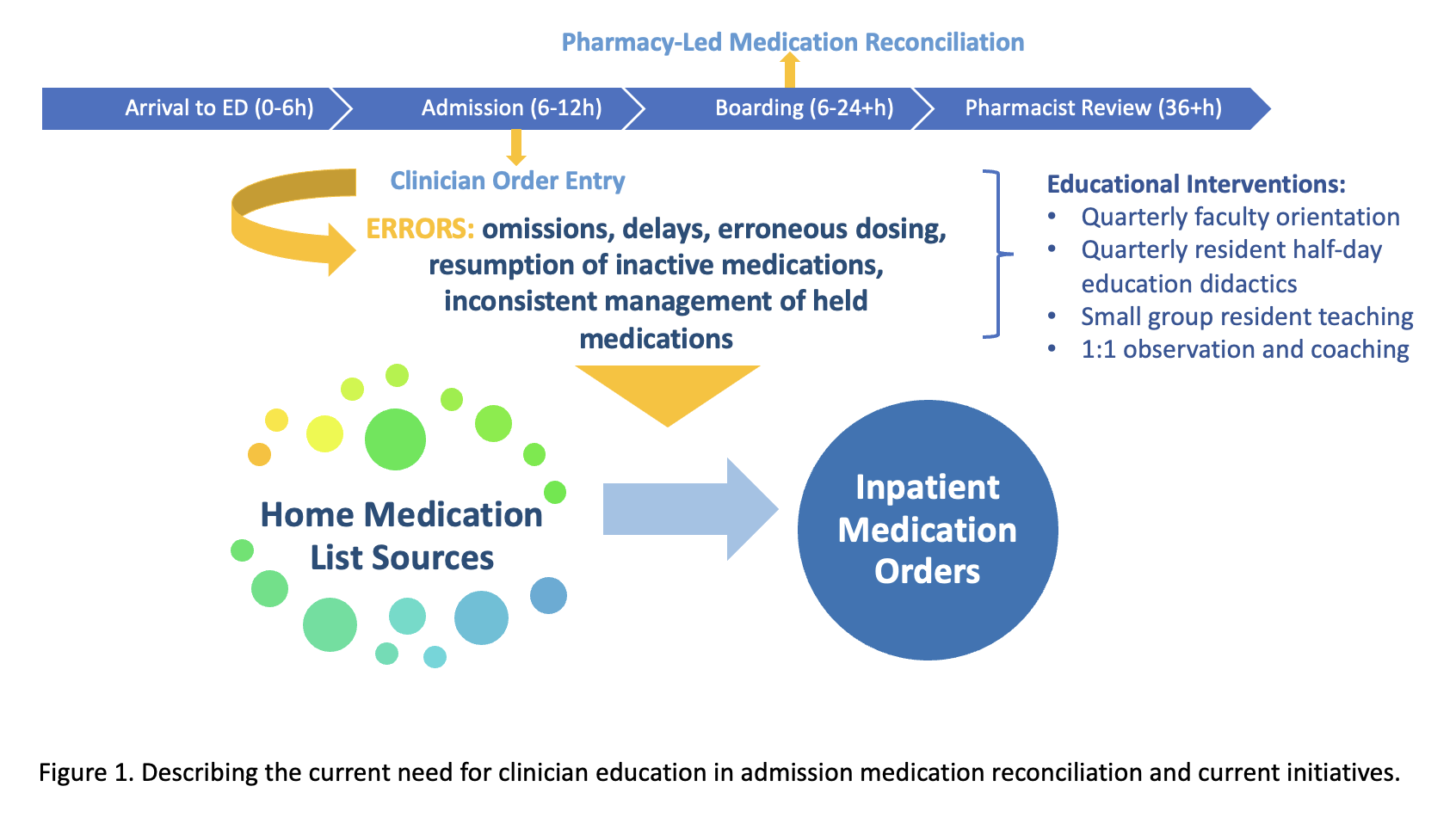
Background: Accurate, timely admission medication reconciliation (AMR) is a key patient-safety driver. Clinician-performed AMR has higher error rates compared to pharmacy-performed AMR. At our large, tertiary care institution, pharmacists capture only 75% of AMRs and require up to 48h for completion. Delays and errors in clinician-performed AMR on medicine floors have led to patient safety events such as excess insulin dosing causing hypoglycemia, resumption of inactive high-dose SNRI leading to excess LOS, and erroneous underdosing of lamotrigine resulting in in-hospital seizure. With the electronic integration of external medication databases into the EMR, improved multi-source medication verification is now possible but requires technological skill and consistent process utilization for both medication history documentation and inpatient ordering. Given the need for rapid AMR at the start of care, the occurrence of AMR-related safety events, and the availability of advanced but underutilized medication databases, we identified a need to enhance competency in clinician-performed AMR.
Purpose: To establish AMR competency for hospitalists and internal medicine (IM) trainees via multipronged educational interventions including interactive resident teaching, real-time AMR observation and coaching paired with Entrustable Professional Activity (EPA) evaluation, and simultaneous hospitalist faculty development.
Description: We developed novel didactics for faculty and residents highlighting: importance of AMR, safety event review, importance of observing/verifying learners’ AMR, live navigation of medication sources, and demonstration of correct AMR process within the EMR (Epic). Learners reviewed AMRs for their own patients during teaching sessions and practiced accessing various sources to corroborate patients’ reported medications. They utilized the admission navigator to practice reconciling medications. Faculty received a demo of the same tools. The didactic sessions were delivered via Teams to hospitalist faculty before an upcoming admitting rotation with interns. IM residents received in-person teaching during educational half-days. Interns received 1:1 AMR training from hospitalists, and attendings submitted evaluations via a novel online EPA (Qualtrics).The effectiveness of this curriculum is being actively evaluated through multiple outcomes, including monitoring AMR-related patient safety events, pre- and post-knowledge assessments, post-didactic feedback, and EPA completion rates with respective competency levels and trends. Preliminary post-assessment data from 26 trainees show an increase in the number of medication resources identified by learners (mean increase from 3.2 to 4.7 resources) and enhanced knowledge of best practices for AMR, as demonstrated by performance on written clinical scenarios.
Conclusions: Dedicated instruction in AMR leverages the unique skill set of hospitalist attendings and addresses a key educational patient-safety gap. The initiative has been well-received by learners and patient-safety stakeholders. We are actively expanding the curriculum into Yale’s Primary Care track, and additional faculty didactic sessions have been requested by non-hospitalist attendings to improve trainee oversight in AMR.