Background: Acute pain crises (APCs) are a common complication of sickle cell disease (SCD) and associated with increased risk of hospitalization and death. Limitations of existing national guidelines in APC acute care management contributes to variability in practices and can result in suboptimal quality of care. To address this area of need, the National Alliance of Sickle Cell Centers (NASCC) conducted a consensus process (6/2022-5/2025) to develop practice standards and recommendations for management of APC.
Methods: NASCC uses a Modified RAND/UCLA Delphi expert panel approach consisting of four phases to develop consensus among its SCD member centers: 1) systematic literature review; 2) panel development of pre-formative statements around both standards and recommendations; 3) hybrid virtual and in-person discussion among stakeholders at NASCC’s annual conferences to refine and approve pre-developed statement definitions; and, 4) final statement revisions and NASCC Center Director voting on standards, and recommendations to be adopted. NASCC uses 2 grades for consensus statements: Standards being that which providers must do to ensure safe and adequate care, or where omission could lead to poor clinical outcomes; Recommendations being those that would be beneficial and that providers should try to follow, but for which there is less evidence. NASCC defined consensus a priori as ≥ 70% of respondents positively endorsing an item (Likert score ≥7, scale 1-9; 1 = highly inappropriate, risks outweigh the benefits and 9 = highly appropriate, benefits outweigh the risks).
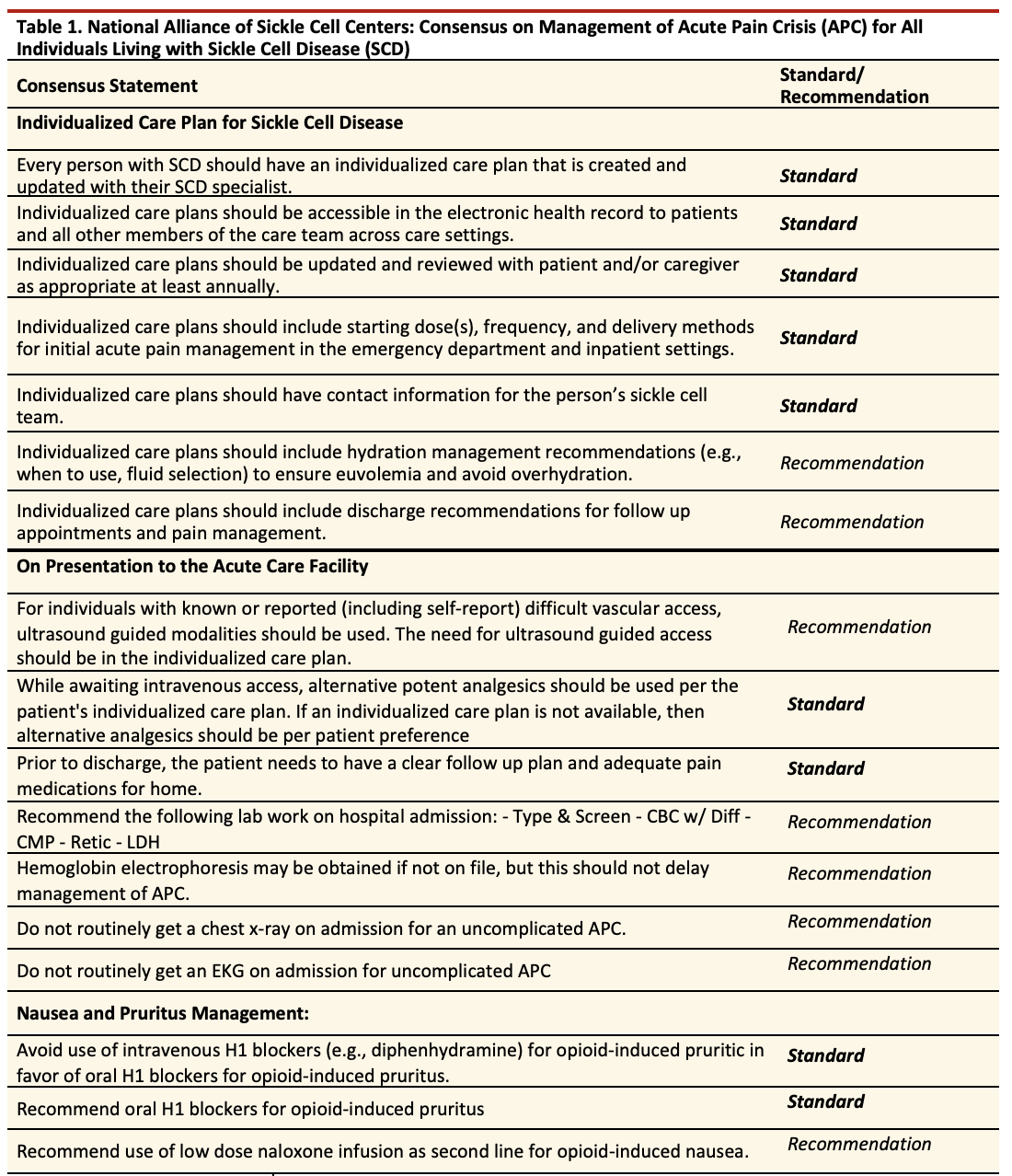
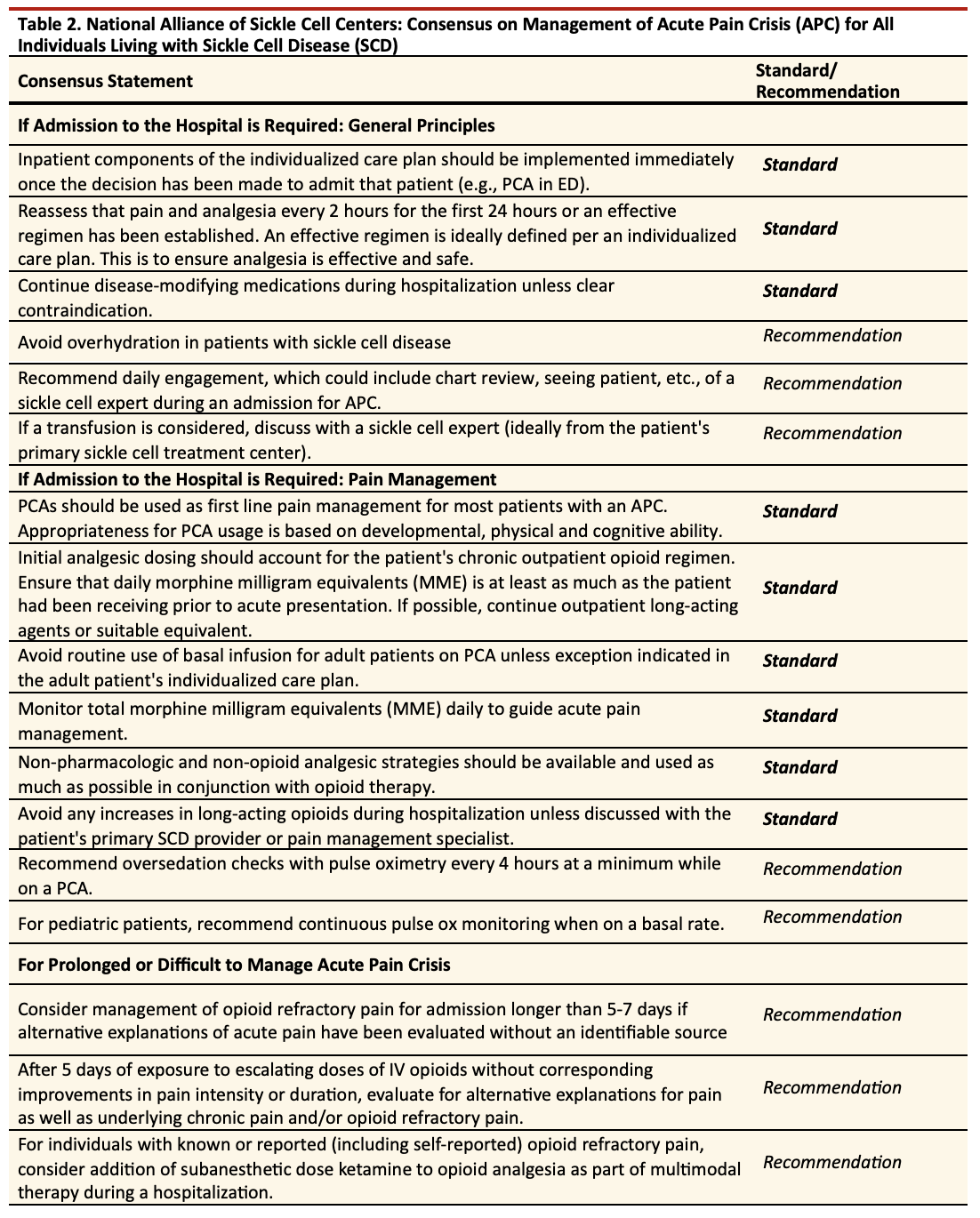
Results: 100 NASCC center directors (87% response rate) voted on 37 consensus statements (19 Standards, 18 recommendations) pertaining to acute care management of APC. Domains included use of individualized care plans (Table 1), initial presentation to an acute care facility (Table 2), and hospital admission (Table 3). Thirty-six statements achieved consensus. Standards included 1) Every person with SCD should have an individualized care plan that includes when and how to context their SCD specialist; 2) Patient-controlled analgesia should be used as first-line pain management for most patients with an APC; 3) Avoid use of intravenous H1 blockers (e.g., diphenhydramine) in favor of oral H1 blockers for opioid-induced pruritus.
Conclusions: Developing evidence-informed consensus on acute care management of APCs for individuals with SCD will allow for practice harmonization in hospital medicine. With decreased care variability, NASCC can test the validity of these consensus statements to inform higher-grade evidence-based guidelines in the future.