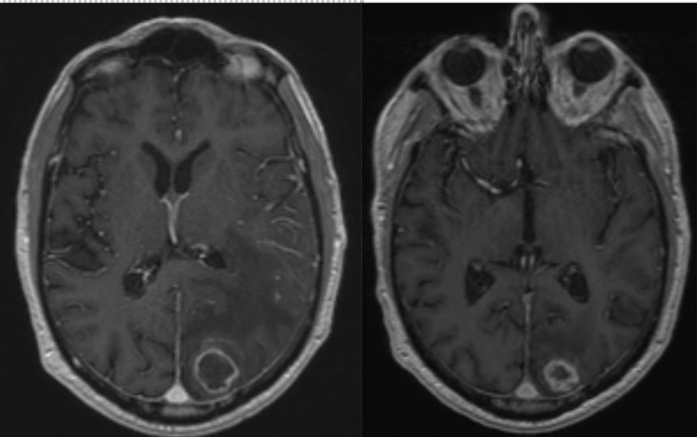
Case Presentation: An 83-year-old man with coronary artery bypass graft, atrial fibrillation, pacemaker, and chronic lymphocytic lymphoma (CLL), presented with a week of dizziness, generalized weakness, blurred vision, word-finding difficulties, and confusion. Dysmetria and peripheral vision loss on the right were notable. No fever. Labs were unremarkable except for mild anemia, lymphocytic leukocytosis, and neutropenia. His CLL was diagnosed 3 years prior; he was initially monitored without treatment. Due to worsening lymphadenopathy, he was then started on Ibrutinib 4.5 months prior to this admission, with good response and no adverse effects. Head CT revealed a 3.7-cm left parieto-occipital mass with surrounding edema and small midline shift, concerning for lymphoma or a new primary malignancy. Ibrutinib was held. Mentation & generalized weakness improved with IV steroid. Brain MRI (left image) showed normal paranasal sinuses, a well-defined, 3 cm left cuneus lesion, favoring intracranial abscess over necrotic metastasis. Neurosurgery performed a biopsy and only a partial evacuation, given the high risks of complete evacuation. Cultures and pathology showed Aspergillus fumigatus. Voriconazole was started. Peripheral blood flow cytometry showed absence of Richter transformation. He was discharged on lifelong oral voriconazole. His blood counts improved. Brain MRI (right image) 3.5 months later showed continued decrease in abscess size.
Discussion: We report a case of a patient with CLL on ibrutinib, with an acute presentation concerning for an intracranial malignancy, and with a final diagnosis of aspergillus brain abscess. A very high index of suspicion is paramount for early diagnosis, especially since CNS aspergillosis has a case fatality as high as 45% (1). The most common risk factors of CNS aspergillosis are corticosteroid use, hematologic malignancy, diabetes, and neutropenia (1). Among hematologic malignancies, CLL is the most common, and among those, ibrutinib is the most common treatment (1). Invasive aspergillosis during ibrutinib treatment commonly presents either as pulmonary, or both pulmonary and CNS (most commonly an abscess, but also meningitis, infarction, or aneurysm) (1,2). Compared to published case series of invasive aspergillosis while on ibrutinib, except for neutropenia, male sex, and CLL diagnosis, our patient was older (83 years old vs reported median ages of 70 years (2) or 65.9 years (3)), the time from ibrutinib initiation to CNS aspergillosis presentation was longer (4.5 months vs reported median times of 2 months (2) or 1.64 months (3)), he had no prior lines of treatment for CLL (including no steroids), no Richter’s transformation, no complex karyotype, and no p53 mutation (2,3). This case thus also suggests a more diverse presentation than captured in recent case series.
Conclusions: This case reminds us of the growing recognition of the association between ibrutinib and invasive aspergillosis especially in the brain. It also highlights atypical features of invasive aspergillosis: CNS involvement alone, absence of systemic manifestations, and later presentation during ibrutinib treatment course. There is a need for heightened suspicion for CNS aspergillosis in patients with cancer presenting with an intracranial mass even without specific signs of infection because early recognition allows for prompt management and better prognosis of this fatal disease.