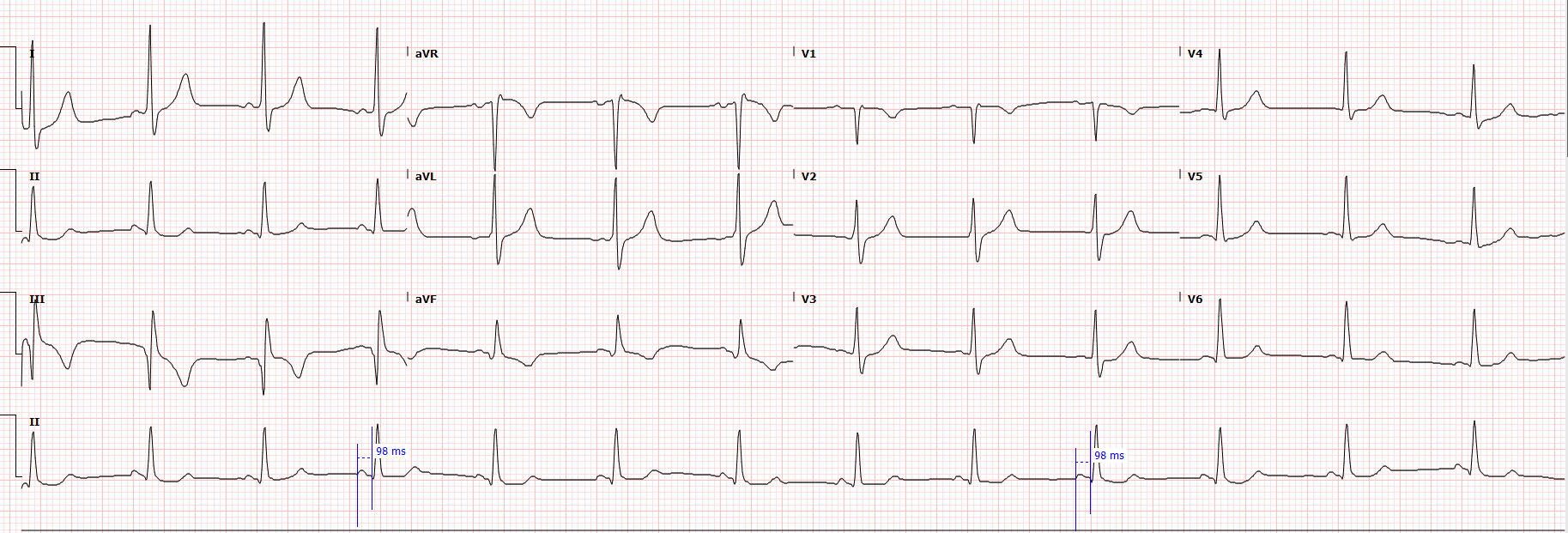
Case Presentation: A 72-year-old man with benign prostatic hyperplasia and a history of paroxysmal atrial fibrillation presented with chest discomfort, dyspnea, dizziness, and weakness. Initial ECG interpretation raised concern for wide-complex tachycardia, prompting further rhythm evaluation. Subsequent telemetry and electrophysiology review identified atypical atrial flutter with variable atrioventricular conduction. His previous cardiac workup had been negative for obstructive coronary artery disease. He was initiated on intravenous amiodarone for rate control and rhythm stabilization, with improvement in symptoms. Detailed review of current and historical ECGs demonstrated a short PR interval (ranging from 90 to 138 ms across more than 10 ECGs) with a normal QRS complex and absence of delta waves, consistent with an unrecognized LGL pattern that had been present on earlier tracings. Of note, there was no prior comment about the short PR interval from the computer interpretation and the overread. The electrophysiology consultant recommended outpatient follow-up with a plan for potential catheter ablation.
Discussion: Lown-Ganong-Levine (LGL) pattern is an uncommon pre-excitation variant characterized by a short PR interval with normal QRS duration and absence of delta waves. Proposed mechanisms include enhanced AV nodal conduction or paranodal fibers enabling rapid atrial-to-ventricular transmission. While many individuals with this pattern remain asymptomatic, LGL physiology may increase susceptibility to supraventricular arrhythmias such as atrial flutter and atrial fibrillation. This case highlights how atypical atrial flutter—and an initial concern for wide-complex tachycardia—can obscure subtle conduction abnormalities on ECG. Early identification of LGL is clinically important because it may help prevent the development of potentially life-threatening arrhythmias through closer rhythm monitoring and timely electrophysiologic intervention.
Conclusions: In patients presenting with complex supraventricular arrhythmias, careful ECG analysis can uncover previously unrecognized conduction patterns such as LGL. Identifying this pattern, especially when present on prior ECGs, can refine arrhythmia management and support appropriate referral for ablation planning. In the intelligent era of AI, there is still a place for human intelligence.