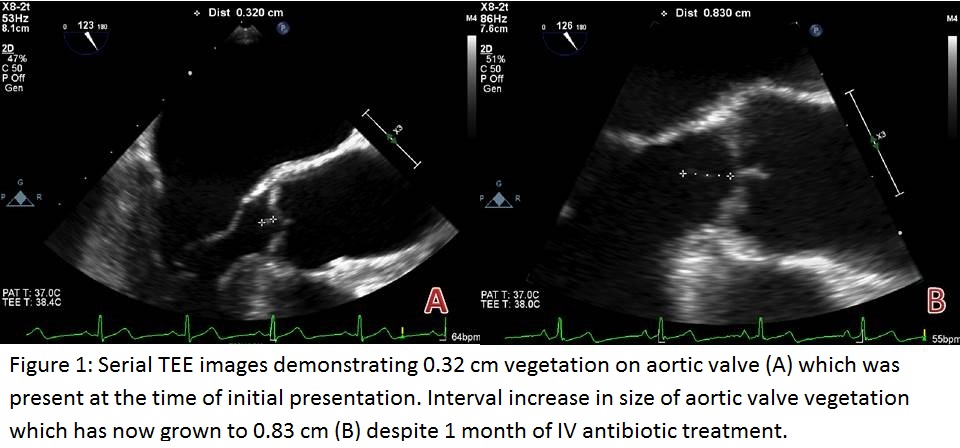
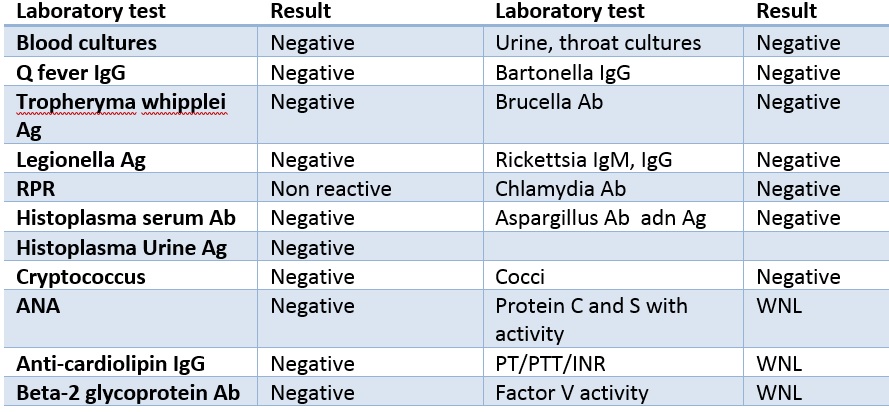
Case Presentation: A 55-year-old female presented with headaches and intermittent fevers. On initial examination, she had left hand weakness. Laboratory findings revealed leukocytosis; brain MRI demonstrated multiple bilateral cerebral infarcts. Initial workup was concerning for embolic stroke which initiated our search for a cardioembolic source. No significant abnormalities were seen on transthoracic echo (TTE) and her blood cultures were negative. During her hospital stay, she was having intermittent fever reaching 103.3 F. Giving high suspicion for embolic source we decided to proceed with trans esophageal echo which revealed multiple small vegetations on the mitral and aortic valves and the diagnosis of endocarditis was made. She was started on IV antibiotics and more blood cultures were obtained. Further blood cultures targeted toward HACEK and fungal organisms, as well as serological testing, were negative. She did not have evidence of malignancy and her autoimmune workup was negative. Repeat TEE one month after her initial presentation revealed enlarged vegetations. Even though the patient has been having a high-grade fever, we decided to stop antibiotics and initiate heparin. Her fever rapidly resolved with heparin and repeated TEE revealed resolution of valvular vegetations.
Discussion: NBTE is an uncommon diagnosis and usually discovered postmortem and is found in 1.2% of patients in autopsy series. It is most commonly associated with malignancy, systemic lupus erythematosus (SLE) and hypercoagulable states, occurring in 4% of all end-stage cancer patients and 11% of SLE patients. The presence of pathological NBTE is a rare condition in patients without cancer diagnosis or autoimmune disease. Diagnosis is very challenging giving the rarity of the disease and close resemblance of other more common valvular and infective diseases. Treatment should involve anticoagulation with heparin rather than warfarin is essential to prevent further thromboembolic complications. The use of DOAC is limited in this disease due to the lack of supporting studies. Surgical intervention is indicated in patients with large vegetations, severe valvular dysfunction, or recurrent embolism despite long term anticoagulation therapy.
Conclusions: NBTE is a rare condition that is commonly associated with malignancy, autoimmune and inflammatory conditions. Our patient presented with NBTE in the absence of malignancy or other causes. Hospitalists should be vigilant for diagnosing and treating this condition especially with endocarditis that is not responding well antibiotic treatment. In addition to addressing the underlying cause, treatment with heparin (or LMWH) rather than warfarin or DOAC is necessary to prevent recurrent embolization.