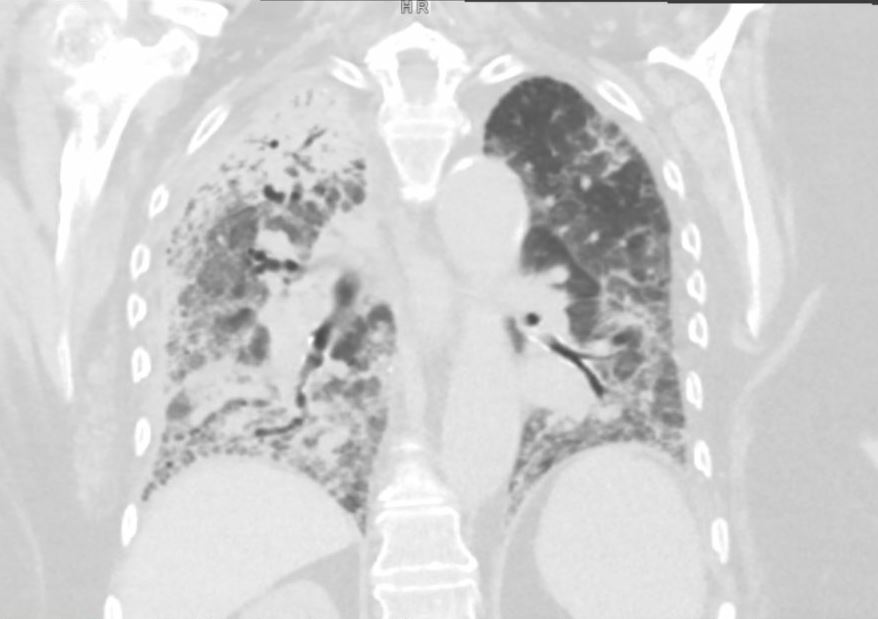
Case Presentation: An 89-year-old female with a history of heart failure with reduced ejection fraction (HFrEF), atrial fibrillation, and prior left atrial appendage occlusion (Watchman) presented with altered mental status and generalized weakness. On admission, she required intensive care unit (ICU) support, including vasopressors and BiPAP for acute respiratory failure and septic shock. She briefly required vasopressor therapy, and was successfully weaned off, though her oxygen requirements remained elevated, necessitating ongoing BiPAP for hypoxia and hypercarbia.The patient remained afebrile but tachycardic, with a predominant rhythm of atrial fibrillation with rapid ventricular response. Initial workup revealed a negative expanded respiratory viral panel. Chest X-ray showed bilateral infiltrates, and a subsequent chest CT identified ground-glass opacities in the right upper, middle, and lower lobes and left lower lobes, concerning for multifocal pneumonia.Blood cultures initially grew Gram-negative rods, later identified as nontypeable Haemophilus influenzae (NTHi), resistant only to trimethoprim-sulfamethoxazole. She was started on empirical vancomycin and piperacillin-tazobactam. Throughout her prolonged six-week hospitalization, the patient experienced intermittent hypoxia, requiring brief ICU transfers for BiPAP. Ultimately, she was weaned to three liters of oxygen and discharged to a rehabilitation facility in a stable condition.
Discussion: Haemophilus influenzae (Hi) is a small, Gram-negative coccobacillus that is classified into two categories: typeable (encapsulated) and nontypeable (nonencapsulated). Typeable serotypes (a–f) were once the leading cause of respiratory infections, particularly in children and older adults. Following the introduction of the Haemophilus influenzae serotype b (Hib) vaccine in 1987, the incidence of Hib infections declined significantly.Recently, however, nontypeable Haemophilus influenzae (NTHi) and serotype A infections have been rising globally, particularly in North America. Nontypeable Haemophilus influenzae has emerged as a prominent pathogen in respiratory infections, and invasive infections, such as bacteremia.In our patient, NTHi was identified as the causative agent of bacteremia from a pulmonary source, leading to a severe clinical course characterized by septic shock, respiratory failure, and protracted hospitalization. This case highlights the severity of infections caused by NTHi, which can be particularly devastating in elderly patients with comorbidities, as seen in our patient with HFrEF and atrial fibrillation.
Conclusions: The epidemiology of Haemophilus influenzae infections has evolved significantly since the introduction of the Hib vaccine. While the incidence of Hib infections has decreased, the rate of Nontypeable Haemophilus influenzae (NTHi) and serotype A infections has risen, particularly in adults over 65 years of age. From 2009 to 2015, the estimated incidence of invasive H. influenzae infections was approximately 1.7 cases per 100,000 population, with the highest rates observed in older adults and young children. The mortality rate for invasive H. influenzae infections, particularly pneumonia, has been reported as high as 22–26%, with the elderly. Hospitalists should be aware of this emerging pathogen as a possible cause of severe pneumonia and septic shock, as early identification and targeted therapy are key to improving outcomes.