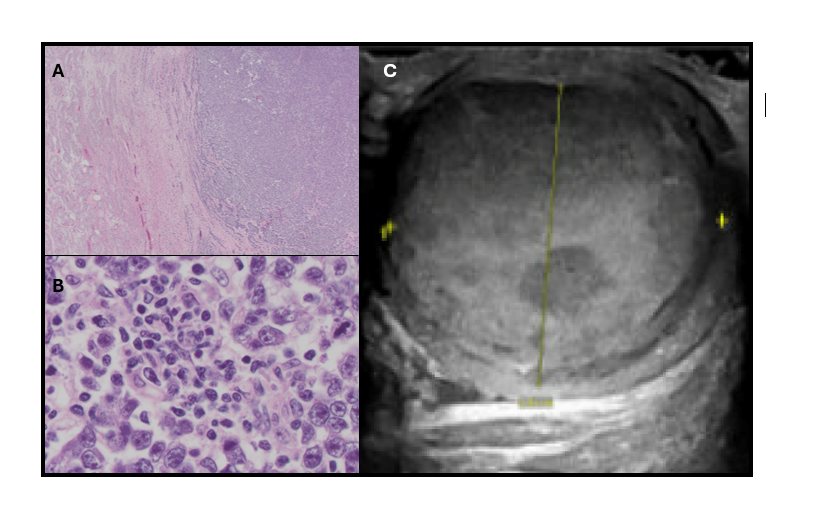
Case Presentation: 26-year-old man diagnosed with T-cell acute lymphoblastic leukemia (T-ALL) with CNS involvement in July 2022 completed one cycle of hyperCVAD B and subsequently received maintenance therapy with POMP (prednisone, vincristine, methotrexate, and mercaptopurine) starting in 2023, along with intrathecal chemotherapy. The patient achieved complete remission, with serial MRIs, PET scans, and bone marrow biopsies remaining negative. During an outpatient follow-up in July 2024, the patient denied new testicular symptoms. However, 1 month later, he reported right testicular firmness, swelling, pain, and back pain, prompting hospital admission. Initial concerns were for focal leukemic infiltrate. A testicular ultrasound revealed a new 4-cm hypervascular mass in the right testis. Serum tumor markers showed low to normal values with, AFP 3.7 ng/ml, LDH 192 U/L, and HCG 1 mIU/mL. Lumbar puncture and bone marrow biopsy results were unremarkable. PET scan revealed testicular uptake. The patient underwent orchiectomy, with pathology confirming a T1b seminoma with negative surgical margins. He will continue active surveillance for testicular cancer, including monitoring serum tumor markers and imaging, as well as complete maintenance therapy for T-ALL.
Discussion: The differential of a testicular mass in this case included recurrent T-ALL versus a primary testis malignancy. T-ALL is rare, given the incidence in the US is 3 cases per million per year. Patients present with cervical, axillary or mediastinal masses (4). “Low” versus “high” risk categories exist depending on certain mutations (7). CNS involvement is common and usually takes the form of leptomeningeal disease (7). In addition to CNS involvement, the testes are also recognized as a sanctuary site in ALL, with testicular relapses reported during or after treatment in B-ALL and rarely in T-ALL (8). Converse to the rarity of isolated testicular T-ALL relapse, testicular cancer is the most common solid malignancy affecting males from 15 to 35 years of age (3). It most commonly presents with a painless or painful testis mass. The diagnostic evaluation includes testicular ultrasound, tumor markers and radical orchiectomy (8, 9). Negative tumor markers do not rule out the diagnosis. Testicular biopsy is contraindicated due to risk of tumor seeding (9). Testicular cancer is highly curable, particularly early-stage seminoma, associated with > 99% 5-year survival following orchiectomy alone (3). Given high cure rates, effective salvage therapy and long-term toxicities associated with additional therapy, the NCCN generally recommends surveillance for Stage I seminoma without additional adjuvant therapy (5, 6).
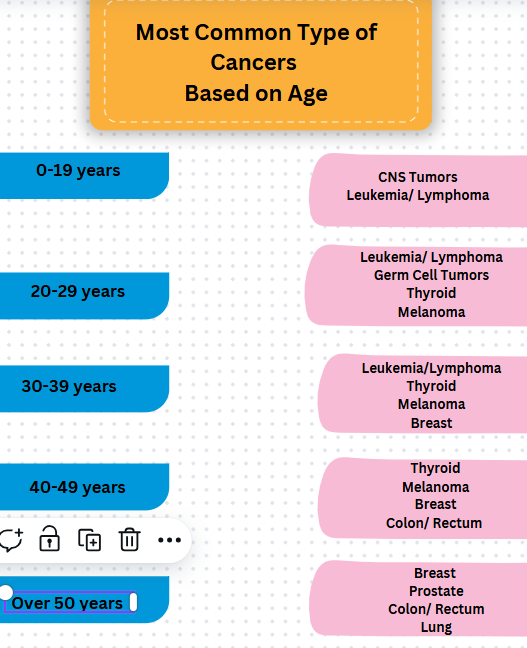
Conclusions: When oncology patients present with symptoms concerning for malignancy, it is essential for hospitalists to have a high index of suspicion for both recurrent malignancy as well as other common malignancies based on patient age and risk factors. Complete work up for recurrent disease as well as other malignancies on the differential can lead to a timely diagnosis with improved outcomes. Primary testicular malignancy should be on the differential of any male with a testicular mass, and initial evaluation includes testicular ultrasound, tumor markers, and, if malignancy is suspected, radical orchiectomy.