Case Presentation:
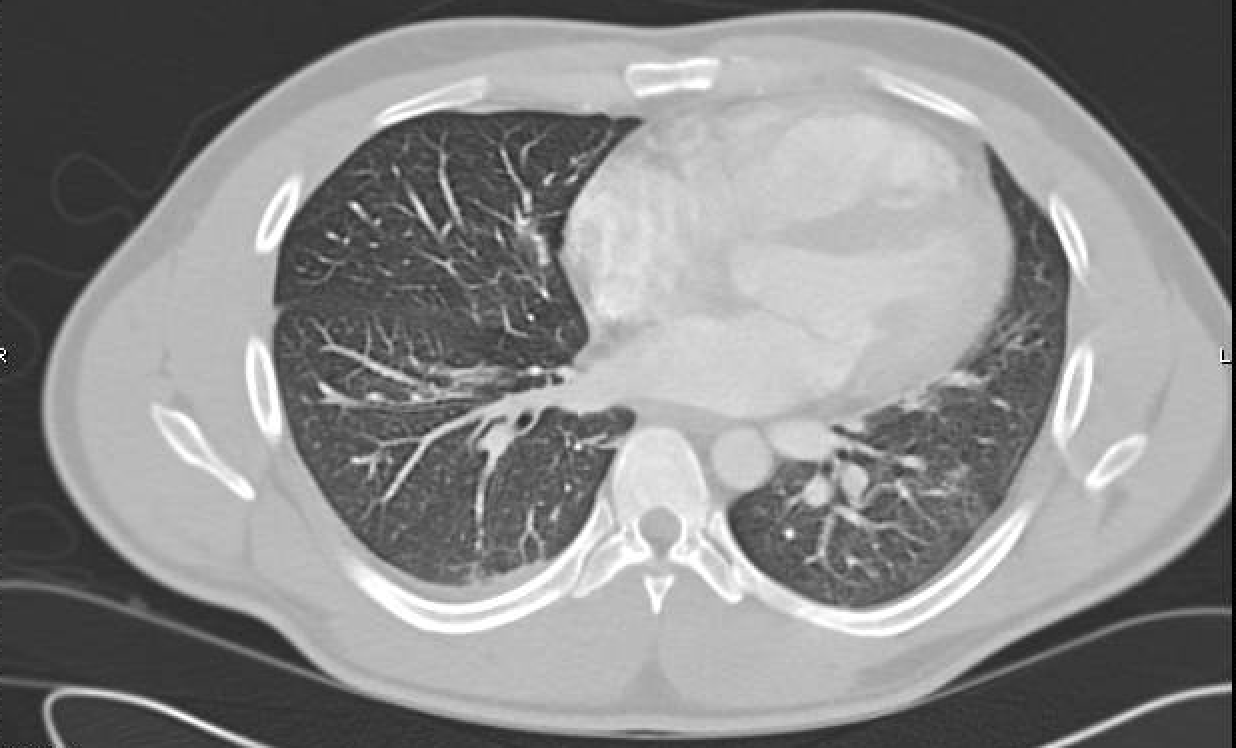
An asymptomatic 27 year-old male with no past medical history presented with an incidental finding of a IV/VI systolic ejection murmur best heard at the left lower sternal border with parasternal heave. Physical examination was otherwise unrevealing with no lymphadenopathy. A subsequent transthoracic echocardiogram revealed a 4 cm by 2.5 cm intracardiac mass firmly attached to the right ventricular outflow tract and pulmonary artery. Computerized tomography (CT) of the chest revealed a mediastinal mass encasing the aorta, aortic arch, trachea, and left mainstem bronchus with significant invasion of the pulmonic valve, and 90% occlusion of the right pulmonary artery. Testicular ultrasound did not reveal any lesions. Thorough infectious workup and tumor markers (bHCG, AFP, CEA, CA 19-9) were both negative. A CT-guided biopsy of the mediastinal mass was performed with histologic examination of the tissue sample showing sclerosis with increased number of plasma cells consistent with IgG4 sclerosing disease and inflammatory pseudotumor. Given the location of the mass, surgical intervention was not indicated. He was started on a course of steroids with close follow-up in Rheumatology and Cardiology clinic. A subsequent CT scan following a 2-month course of steroid therapy showed interval decrease in the size of the mass. Physical examination on follow-up demonstrated a decrease in the intensity of the systolic murmur. The plan was to continue on steroid therapy with interval CT scans.
Discussion:
Inflammatory pseudotumors are described as non-neoplastic growth of inflammatory cells that appear like malignancy on radiographic imaging and can rarely be IgG4 positive. IgG4-related disease is an immune mediated inflammatory disease characterized by a unique histopathologic appearance and mass formation that imitates malignancy. It may occur in any site of the body but is rarely observed in the mediastinum. Although surgical removal of the mass is the first line of treatment, in uncommon cases where the inflammatory pseudotumor is secondary to IgG4 related disease the preferred treatment is steroids. In such a scenario, as in the case of our patient, response is monitored with interval imaging and continued steroid treatment. While spontaneous improvement has been observed, most patients have relapses following cessation of steroid therapy.
Conclusions:
It is critical that in patients with an observed mediastinal mass to differentiate IgG4-related disease from other malignant masses as it dictates the ultimate treatment approach. Biopsy is necessary to confirm diagnosis and interval CT scans should be used to monitor response following initiation of steroid therapy.