Background: The opioid epidemic is a national health crisis, and veterans in particular, at increased risk for developing substance use disorders. The use of medications for treatment of opioid use disorder (MOUD) is a life-saving, cost-effective intervention. However, MOUD is consistently underutilized, particularly in the inpatient setting and little has been published regarding Veterans Affairs (VA) inpatient MOUD interventions. Inpatient methadone maintenance initiation is fraught with barriers due to regulatory concerns, dosing complexities, side effect profile and the need for bridging to certified outpatient Opioid Treatment Programs. Fewer hurdles exist for buprenorphine/naloxone maintenance. We sought to determine whether implementation of a phased quality improvement (QI) initiative would lead to increased MOUD prescribing and optimize treatment for hospitalized veterans with opioid use disorder (OUD).
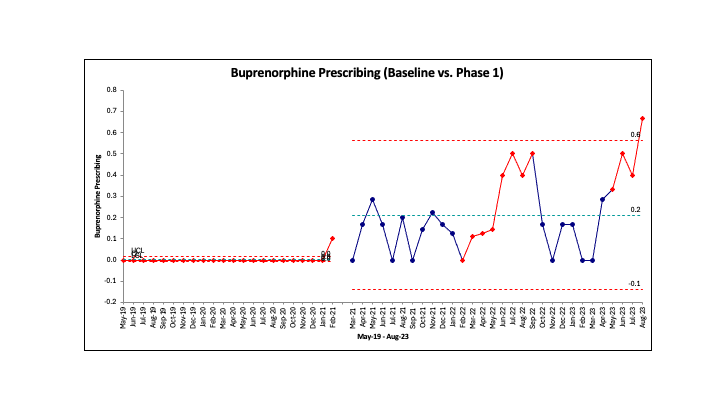
Methods: In January of 2021, a hospitalist-led multidisciplinary team including addiction specialists, psychiatry, nursing, pharmacy, and social work, created a two-phased quality improvement initiative aimed at optimizing treatment for hospitalized veterans admitted with OUD. Phase 1 (March 2021-August 2023) consisted of hospitalist-targeted OUD and MOUD educational sessions, hospitalist-driven buprenorphine/naloxone prescribing, and creation of a dedicated buprenorphine/naloxone order set to aid in prescribing. Phase 2 (September 2023-December 2024) included obtaining institutional approval for, and initiation of an inpatient addiction consult team. A split limit analysis was performed to assess for differences in buprenorphine/naloxone prescribing trends.
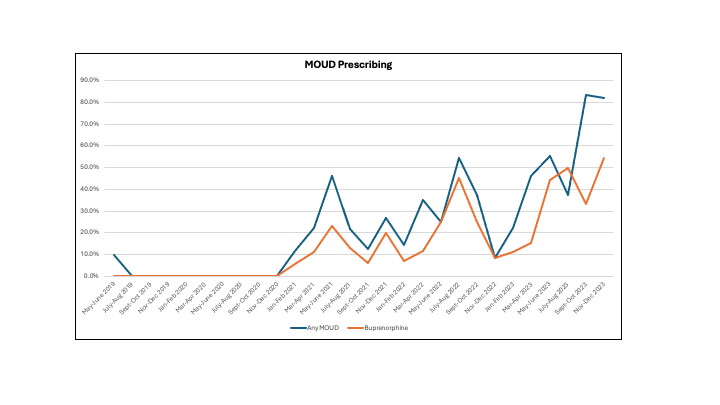
Results: We reviewed prescribing trends at our urban, 200-bed acute care VA hospital from May 2019 through December 2023, which encompassed Phase 1 and the beginning of Phase 2. Full analysis of Phase 2 is in process. A total of 244 hospitalizations of MOUD-naïve patients with OUD are currently included. Our patient population was primarily older (65.9 ± 7.8), male (95.0%), Black and/or African American (87.1%), and not Hispanic or Latino (92.1%). The majority of patients, 81.2%, had one or more co-substance use disorders (78.0% tobacco, 47.6% cocaine, and 40.2% alcohol) and housing insecurity impacted 43.6%. At baseline (May 2019-February 2021), an average of 2.3% of inpatients with OUD were discharged with MOUD, with 0.8% receiving buprenorphine/naloxone. In Phase 1 hospitalists were encouraged to begin prescribing buprenorphine/naloxone to treat inpatients with OUD, and a dedicated order set to aid in prescribing was launched in July 2022. During Phase 1, the percentage of inpatients with OUD receiving MOUD on discharge increased to an average of 33.0%, with buprenorphine/naloxone prescribing rising to 19.4%. Though final Phase 2 analysis is still in progress, early results show that under the addiction consult service MOUD prescribing increasing further to 89.4%, with 36.4% of patients receiving a buprenorphine formulation. Figures 1 and 2 demonstrate changes in MOUD prescribing over time.
Conclusions: We found that a phased, hospitalist-led QI initiative increased inpatient total MOUD and buprenorphine prescribing over time. Early results suggest that addition of a dedicated inpatient addiction consult team further augments OUD treatment optimization.