Background: Patient experience metrics heavily impact healthcare institutions’ rankings, reputations, and funding. Prior research has shown that 92% of patients consider “listening to you” to be very or extremely important, ranking third in importance after clear communication and being treated with courtesy and respect (The Beryl Institute, 2024). However, few studies have explored what behaviors make patients feel heard (Roos, 2023). At the hospital in this study, only 51.6% of 519 hospital medicine patients rated providers in the top box for “listening carefully” (January 2024 – July 2025) compared to 91.3% in Radiation Oncology, the top-scoring division. This study aims to identify best practices that help patients feel listened to and the barriers to implementing them to design quality improvement projects that will reduce existing gaps.
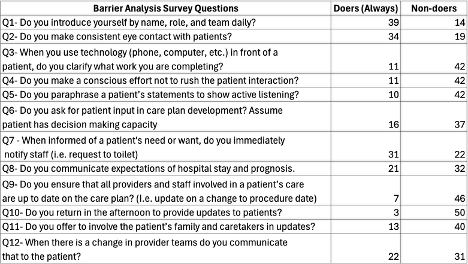
Methods: To understand patient preferences for “feeling listened to”, the research team reviewed 239 patient comments from HCAPS, interviewed 52 randomly selected patients in the medicine service, and surveyed 15 former patients. 12 best practices for “listening carefully” were identified based on survey responses, patient interviews, and literature review. The research team then surveyed hospital medicine providers via a digital questionnaire, using a barrier analysis framework, to assess the use of these practices and barriers to their implementation (Kittle, 2017). Providers who selected “always” for performing a best practice were classified as “doers”. Alternatively, those who selected “Often”, “Sometimes”, “Rarely”, or “Never” were “non-doers”. Non-doers were asked to identify barriers to execution, including perceived importance of the action, time constraints, competing responsibilities, insufficient resources, frustration or low satisfaction, lack of skills, or other. Doers were not asked about barriers to minimize survey attrition from excessive length. Lastly, responses were analyzed using a well-established Barrier Analysis Tabulation Sheet to calculate the statistical significance of each barrier.
Results: Of 212 eligible hospitalists, 53 completed the barrier analysis survey. Most recognized the importance of all 12 best practices. Two best practices had the highest rates of inconsistent application. The first was “Patients feel carefully listened to when providers clarify why they are using technology in front of them”. 79% of hospitalists were non-doers, 43% cited time restraints (p=0.008), and 48% cited competing responsibilities (p = 0.004). The second was “Patients feel carefully listened to when providers return in the afternoon to provide updates”. 95% of hospitalists were non-doers, 76% cited time restraints (p=0.005), and 72% cited competing responsibilities as barriers (p=0.009).
Conclusions: Hospitalists understand best practices for listening, but implementation is hindered by time and competing priorities. Targeted interventions addressing these barriers, particularly for technology use and afternoon updates, may enhance provider listening and patient experience.
.png)